
The FST Trauma Safety Playbook
I will never forget the phone call. Sarah, a highly competent trauma therapist, contacted me and said:
Scott, I am stuck with this family. I have been seeing them for over ten months with little to no significant change. Fifteen-year-old Leon is now involved in both the juvenile justice system for stealing a car and also the child welfare system. Leon’s single-parent mom, Juanita, has not paid utilities in months, there is no bed for him to sleep on and little food in the house. As a result, he and his three younger brothers are at risk for placement into foster care. Even worse, Juanita is clinically depressed, Leon refuses to attend school, and does not show up for his probation community services classes. I have also been unable to engage Leon’s dad or Juanita’s current boyfriend. I left one voicemail for the dad with no return call and the boyfriend is not responsive. For the last ten months, I have been seeing Juanita individually for her depression and providing parenting tools for Leon and his siblings. But I can’t figure out why it’s not working, and the family is falling deeper into crisis. Can you help?
What Went Wrong?
This situation is a vital case description regarding the importance of safety first. Within the FST | Family Systems Trauma Model, the trauma therapist must decide between:
- Stabilize safety first (i.e., parent-child conflict, neglect issues, extreme acting out child behaviors, self-harm, drug abuse, bullying, etc.),
or
- Active trauma treatment first (i.e., unresolved grief, abandonment, family secrets, anxiety, lack of nurturance, etc.).
We discuss this important decision in greater detail using what is called the “three rules of thumb” in the article entitled: FST Stabilization vs. Active Trauma Technique: Setting the Goals of Therapy.
I compare this safety stabilization vs. active trauma first choice to the decisions emergency room doctors must make when a patient with a bleeding gunshot wound enters the ER. The doctor must quickly assess what to do first: stop the bleeding or remove the bullet? The bleeding represents the immediate safety concerns, and the bullet represents the cause of the trauma. A wrong decision can curtail the healing process or even cost the patient his or her life.
My colleague Sarah was stuck with Leon’s case because safety first was not addressed in two specific areas:
#1. Hierarchy of Need Safety Violations
The first reason was Sarah’s tactical decision to focus on this family’s trauma or psychological needs (i.e., parenting skills, depression, parent-child relationships, etc.) without first addressing the family’s basic safety needs of food, clothing, and shelter.
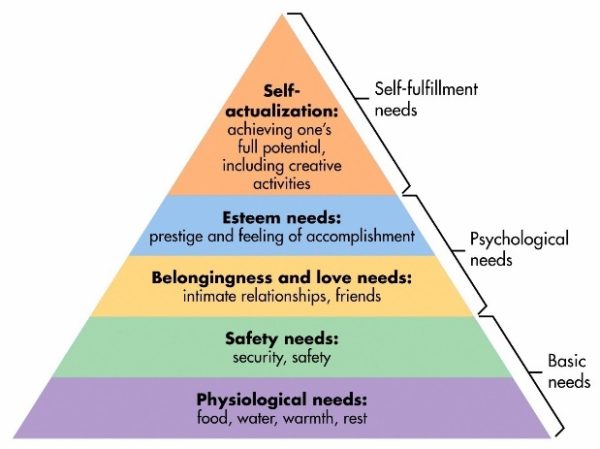
This relationship between basic vs. psychological needs is illustrated through Maslow’s Hierarchy of Needs or the five-tier model of human needs shown in Figure 1. Maslow states that individuals must achieve basic needs first (physiological and safety) before moving to higher needs, such as psychological or self-fulfillment.
In turn, when safety needs are neglected, problem symptoms and negative repercussions take place. In Leon’s case, not having a bed to sleep on or adequate food led to a chain reaction of sleeping in class, an inability to focus, negative attitudes by his teachers, and getting further behind academically. Leon then had no interest in attending school or reason to go to his probation community services classes.
In addition, there is now a high risk for removal by Child Protective Services (CPS) due to neglect issues from a lack of basic needs, not physical or mental abuse.
Sarah, however, focused on active trauma treatment surrounding the mom’s clinical depression and parent-child conflict using behavioral modification contracts.
The mother was labeled as clinically depressed. But a better reframe is that her depression was a normal reaction to being overstressed and overwhelmed. We would also be depressed if we had no job, experienced housing insecurity, and dealt with the risk that our children might be removed for neglect.
In short, Leon’s family needed stabilization first through safety planning but instead received a steady dosage of trauma treatment to address Maslow’s psychological needs of esteem, love, and belonging.
Timing is everything. And the timing was a misfire for Leon’s family.
#2. A Lack of a Written Trauma Playbook
Leon’s family needed a written safety first plan of action that involved paying for the utilities and mobilizing a support system before the mother, Juanita, could muster the energy or bandwidth to address psychological trauma with herself and her children.
What was needed was a “town meeting” approach where the mother, the father, the boyfriend, the caseworker, the probation officer, and any extended family or friends are brought together in one room with clear directions to create a written plan of action to “get the lights on” and to support the mother and entire family.
At the Family Trauma Institute and within the FST treatment model, we developed what are called FST Safety Trauma Playbooks. This type of safety trauma playbook was used to help unstick Leon’s family. Please see Chapter 8 of Treating the Traumatized Child: A Step-by-Step Family Systems Approach for procedures of how to create these types of playbooks for your cases.
In sum, Leon’s family and Sarah remained stuck within this second area based on the following reasons:
- Sarah saw Juanita and Leon individually instead of mobilizing the boyfriend, caseworker, probation officer, and local pastor in a “town meeting” to help mom and son. The extended family was never contacted in the entire ten months of treatment. Sarah lacked family systems trauma training. As a result, she treated the case using a non-systemic lens.
- Juanita desperately needed assistance to get the utilities on, food, and a bed for Leon. Sarah provided the mom with community referral information. However, the mom lacked the energy, expertise, or bandwidth to do this on her own. The therapist was well-intentioned but did not have the tools to organize a family therapy session to create a safety trauma playbook.
The definition of insanity is doing the same thing over and over again, even though it doesn’t work. In Leon’s case, the definition of insanity was keeping this family traumatized and stuck.
How the Case Was Unstuck Using FST Safety Planning
As a consultant, the first thing I did was to assess with Sarah and the family their current safety levels.
Step 1: Assess Current Safety Levels
To accomplish this goal, the FST therapist uses a verbal safety risk scale of 1 to 5 (1= no risk; 5 = high risk). If the parents or child state that the risk level is currently high at “3” or above, the FST therapist is faced with an important decision:
- Postpone moving forward into active trauma treatment until the risk level has dropped to lower than a 3.
This simple risk level scaling is an ideal first step to bring quick and efficient insight for both the family or the therapist to slow down with a safety first rating or to process forward with active trauma treatment if the risk level is a “3” or below.
In Leon’s family, everyone stated that they were at a “5” with mom shutting down due to her depression and the possibility of the kids being placed in temporary foster care.
Step 2: Get the Right People on the Bus
In the article entitled, How to Engage the Extended Family in Trauma Treatment, I describe the importance of “who” before “what”.
We should shift our decision [in safety planning] from a “what” question (“What should we do?”) to a “who” question (“Who would be the right person to take responsibility for this?”). Translated into treatment, this means that the therapist should spend more time on the “who” decision before launching into the “what” of treatment. It is crucial to get the right people on the bus in the right seats and the wrong people off the bus. First, we focus on the people, then the direction.
Translation: Sarah did not have the right people on this family’s bus or “the who” before “the what”. Having the right people on the bus in treatment is absolutely a critical first step in safety planning. Juanita was trying to pull the family metaphorically out of the mud with one therapist visiting one time per week and with children who had out of control behaviors. She was all alone and had no clear written plan of action.
High safety risk = crisis. When a child or family is in crisis, it is not a time for problem exploration but a time for action.
I used the techniques of the FST Motivational Phone Call and the FST Diagnostic Village Handout to quickly engage and bring together all of the key extended family members.
Step 3: Construct an FST Family Systems Playbook
When everyone was assembled, we used this FST Safety Trauma Playbook to clarify everyone’s roles within a “who, what, when, where, and how?” format.
Please note the following:
- This format allows for clarity of everyone’s role and how to realign and pull together as one team to address the safety crisis at hand. In this case, it was the need for utilities and bedding for Leon.
- In turn, the risk for CPS removal was eliminated, and the mother’s depression was remarkably better because she finally had the support that is both clear and measurable with accountability.
- Leon, in turn, started performing well in school and attending his juvenile probation community service obligations. Without the extended family and the playbook, it is unlikely that his family would decrease the safety risk below a Level 3 and get unstuck.
Conclusion
After the playbook was implemented, the family was again asked the verbal safety risk scale of 1 to 5. The mother and children now said that it was at a “2”. Mom still needed parenting tools, but her depression was lifting, and her energy and motivation had returned. In turn, with the dad now involved, Leon was like a different child. The table was now set to do active trauma and psychological treatment once stabilization was achieved with safety levels below a “3”. The case got unstuck after we knew where to tap and how to tap using a Family Systems Trauma framework.
About the Author
Scott P. Sells, Ph.D., MSW, LCSW, LMFT, is the author of three books, Treating the Tough Adolescent: A Family-Based, Step-by-Step Guide (1998), Parenting Your Out-of-Control Teenager: 7 Steps to Reestablish Authority and Reclaim Love (2001), and Treating the Traumatized Child: A Step-by-Step Family Systems Approach (2017). He can be contacted at spsells@familytrauma.com or through LinkedIn and Facebook.

buy lorazepam 2mg usa pharmacy
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
M88lu has proven to be a very informative website. I read a lot about betting and playing, it gave me a lot of insights to win. So better check it out maybe m88lu can help you too!
V9betxa is just perfect! The odds are very high, and I won a lot of times already. The community is also very helpful with their tips and tricks. You can visit v9betxa if you wanna start earning.
Who doesn’t love free stuff, right? Finding a working Okbet redeem code is like hitting the jackpot! Keep an eye out, they pop up now and then. Hope you get a okbet redeem code free!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://accounts.binance.com/es-AR/register?ref=UT2YTZSU
Понятие гедонизма — это направление в философии, которое рассматривает приятные ощущения в центр человеческой жизни.
Согласно этому взгляду, поиск радости считается значимой частью существования.
Этот подход не всегда подразумевает отсутствие ограничений.
Во многих трактовках он связан с умеренностью и осознанный выбор.
https://telegra.ph/Jacquemus-12-25
Современное понимание гедонизма часто акцентирует внимание на качестве жизни.
При этом важную роль играет гармония между удовольствиями и обязанностями.
Гедонистический подход может способствовать личному развитию.
В итоге, гедонизм рассматривается как один из способов осмысления жизни, а не как отказ от ответственности.
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
Your article helped me a lot, is there any more related content? Thanks!
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.com/register?ref=IHJUI7TF
Your article helped me a lot, is there any more related content? Thanks!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.com/sk/register?ref=WKAGBF7Y
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://www.binance.info/register?ref=IXBIAFVY
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
**back biome**
Backbiome is a naturally crafted, research-backed daily supplement formulated to gently relieve back tension and soothe sciatic discomfort.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.info/es-AR/register?ref=UT2YTZSU
**prodentim**
ProDentim is a distinctive oral-care formula that pairs targeted probiotics with plant-based ingredients to encourage strong teeth, comfortable gums, and reliably fresh breath.
**neurosharp**
Neuro Sharp is a modern brain-support supplement created to help you think clearly, stay focused, and feel mentally confident throughout the day.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me? https://www.binance.com/en-ZA/register?ref=B4EPR6J0
HeroUP is a premium mens wellness formula designed to support sustained energy, physical stamina, and everyday confidence.
Mitolyn is a carefully developed, plant-based formula created to help support metabolic efficiency and encourage healthy, lasting weight management.
Boostaro is a purpose-built wellness formula created for men who want to strengthen vitality, confidence, and everyday performance.
Arialief is a carefully developed dietary supplement designed to naturally support individuals dealing with sciatic nerve discomfort while promoting overall nerve wellness.
Maintaining prostate health is crucial for men’s overall wellness, especially as they grow older. Conditions like reduced urine flow, interrupted sleep
InsuLeaf is a high-quality, naturally formulated supplement created to help maintain balanced blood glucose, support metabolic health, and boost overall vitality.
ProDentim is a distinctive oral-care formula that pairs targeted probiotics with plant-based ingredients to encourage strong teeth, comfortable gums, and reliably fresh breath.
Manergy is an advanced male vitality supplement created to help support healthy testosterone levels
PurDentix is a revolutionary oral health supplement designed to support strong teeth and healthy gums. It tackles a wide range of dental concerns
NerveCalm is a high-quality nutritional supplement crafted to promote nerve wellness, ease chronic discomfort, and boost everyday vitality.
Gluco6 is a natural, plant-based supplement designed to help maintain healthy blood sugar levels.
Nitric Boost Ultra is a daily wellness formula designed to enhance vitality and help support all-around performance.
NerveGenics is a naturally formulated nerve-health supplement created to promote nerve comfort, cellular energy support, antioxidant defense
ProstAfense is a premium, doctor-crafted supplement formulated to maintain optimal prostate function, enhance urinary performance, and support overall male wellness.
Kerassentials is an entirely natural blend crafted with 4 potent core oils and enriched by 9 complementary oils and vital minerals.
MounjaBoost is a next-generation, plant-based supplement created to support metabolic activity, encourage natural fat utilization
NativeGut is a precision-crafted nutritional blend designed to nurture your dog’s digestive tract.
GL Pro is a natural dietary supplement formulated to help maintain steady, healthy blood sugar levels while easing persistent sugar cravings.
Prostadine concerns can disrupt everyday rhythm with steady discomfort, fueling frustration and a constant hunt for dependable relief.
ViriFlow is a dietary supplement formulated to help maintain prostate, bladder, and male reproductive health. Its blend of plant-based ingredients is designed to support urinary comfort and overall wellness as men age.
Visium Pro is an advanced vision support formula created to help maintain eye health, sharpen visual performance, and provide daily support against modern challenges such as screen exposure and visual fatigue.
Backbiome is a naturally crafted, research-backed daily supplement formulated to gently relieve back tension and soothe sciatic discomfort.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
prednisone 10 mg tablets: prednisone – online prednisone 5mg
prednisone 10mg: SteriCare Pharmacy – prednisone 5mg coupon
https://northaccessrx.com/depression-treatments.html# canada rx pharmacy world
discount pet meds: Paw Trust Meds – Paw Trust Meds
pharmacy wholesalers canada: reddit canadian pharmacy – www canadianonlinepharmacy
Paw Trust Meds: pet meds for dogs – Paw Trust Meds
https://pawtrustmeds.shop/# Paw Trust Meds
Global India Pharmacy: п»їlegitimate online pharmacies india – top online pharmacy india
https://northaccessrx.shop/# canadian pharmacy uk delivery
best canadian pharmacy to buy from: canadian pharmacy – canada drugs online reviews
Global India Pharmacy: Global India Pharmacy – best india pharmacy
https://globalindiapharmacy.shop/# Global India Pharmacy
indianpharmacy com: Global India Pharmacy – Global India Pharmacy
canadian pharmacy 24h com: 77 canadian pharmacy – reputable canadian pharmacy
onlinecanadianpharmacy: NorthAccess Rx – cheapest pharmacy canada
https://northaccessrx.com/otc-meds.html# canadian pharmacy world reviews
https://globalindiapharmacy.com/# online pharmacy india
the canadian pharmacy: NorthAccess Rx – safe canadian pharmacy
canadian pharmacies: NorthAccess Rx – canadian online pharmacy
https://globalindiapharmacy.shop/# Online medicine home delivery
Global India Pharmacy: Global India Pharmacy – indian pharmacy paypal
canadian pharmacy ltd: NorthAccess Rx – canadianpharmacyworld
Global India Pharmacy: Global India Pharmacy – indianpharmacy com
https://pawtrustmeds.com/# п»їdog medication online
https://globalindiapharmacy.com/# top online pharmacy india
dog prescriptions online: online pet pharmacy – dog prescriptions online
canadapharmacyonline legit: pharmacy rx world canada – canadian pharmacy store
online pet pharmacy: Paw Trust Meds – Paw Trust Meds
https://northaccessrx.com/antibiotics-guide.html# canadian pharmacy 365
Global India Pharmacy: Global India Pharmacy – buy prescription drugs from india
pet pharmacy online: vet pharmacy – vet pharmacy
mail order pharmacy india: Global India Pharmacy – Global India Pharmacy
https://northaccessrx.shop/# legitimate canadian online pharmacies
canada online pharmacy: canadian pharmacy online reviews – pharmacy wholesalers canada
pet meds for dogs: Paw Trust Meds – pet prescriptions online
NerveCalm is a high-quality nutritional supplement crafted to promote nerve wellness, ease chronic discomfort, and boost everyday vitality.
Global India Pharmacy: Global India Pharmacy – Global India Pharmacy
PurDentix is a revolutionary oral health supplement designed to support strong teeth and healthy gums. It tackles a wide range of dental concerns, including gum inflammation and tooth decay
AquaSculpt is a high-quality metabolic support supplement created to help the body utilize fat more efficiently while maintaining steady
GL Pro is a natural dietary supplement formulated to help maintain steady, healthy blood sugar levels while easing persistent sugar cravings.
https://globalindiapharmacy.com/# Global India Pharmacy
Boostaro is a modern mens wellness formula created to support daily vitality, stamina, and confidence through a practical, natural routine.
Backbiome is an advanced daily wellness supplement formulated to help support spinal comfort, reduce feelings of built-up tension, and promote freer, smoother movement throughout everyday life.
onlinepharmaciescanada com: canada ed drugs – canadian pharmacy online reviews
Paw Trust Meds: Paw Trust Meds – pet pharmacy online
online canadian pharmacy review: NorthAccess Rx – canadian pharmacy price checker
Global India Pharmacy: Global India Pharmacy – top online pharmacy india
Global India Pharmacy: Global India Pharmacy – Global India Pharmacy
canadian pharmacy meds reviews: NorthAccess Rx – best canadian pharmacy
Paw Trust Meds: discount pet meds – vet pharmacy
http://globalindiapharmacy.com/# Global India Pharmacy
http://pawtrustmeds.com/# Paw Trust Meds
Online medicine home delivery: Global India Pharmacy – Global India Pharmacy
Global India Pharmacy: best online pharmacy india – indian pharmacy paypal
Global India Pharmacy: online shopping pharmacy india – india pharmacy mail order
sildenafil over the counter: CoreBlue Health – viagra canada
sure save pharmacy: canadian pharmacy 24 – polish pharmacy online uk
canadian mail order pharmacy CivicMeds п»їcanadian pharmacy online
https://veritascarepharm.shop/# VeritasCare
online canadian pharmacy coupon: CivicMeds – trusted online pharmacy
https://veritascarepharm.com/# VeritasCare
VeritasCare: VeritasCare – Generic Cialis without a doctor prescription
Buy Tadalafil 5mg п»їcialis generic Buy Tadalafil 10mg
list of online pharmacies: CivicMeds – reputable online pharmacy no prescription
canadian pharmacy generic viagra: CivicMeds – online pharmacy pain
VeritasCare п»їcialis generic VeritasCare
https://civicmeds.com/# canadian pharmacy 365
online pharmacies that use paypal: CivicMeds – legitimate online pharmacy usa
the canadian pharmacy: super saver pharmacy – my canadian pharmacy reviews
legitimate canadian pharmacies CivicMeds legitimate canadian mail order pharmacy
https://veritascarepharm.com/# VeritasCare
CoreBlue Health: CoreBlue Health – cheapest viagra
canadian pharmacy no prescription: canadian valley pharmacy – discount pharmacy online
http://veritascarepharm.com/# VeritasCare
canadian pharmacy mall no rx needed pharmacy online pharmacy reviews
Your article helped me a lot, is there any more related content? Thanks!
Viagra online price: CoreBlue Health – CoreBlue Health
VeritasCare: VeritasCare – VeritasCare
CoreBlue Health cheapest viagra sildenafil online
https://veritascarepharm.com/# Cialis 20mg price
CoreBlue Health: Viagra online price – Generic Viagra online
https://civicmeds.com/# online pharmacy australia
best canadian pharmacy no prescription: CivicMeds – canadian online pharmacy
Cheap Cialis VeritasCare VeritasCare
CoreBlue Health: Viagra tablet online – sildenafil 50 mg price
canadian online pharmacy: CivicMeds – canadian pharmacy 365
CoreBlue Health CoreBlue Health Generic Viagra online
https://veritascarepharm.shop/# VeritasCare
medstore online pharmacy: CivicMeds – online pharmacy fungal nail
VeritasCare: Cialis 20mg price – Buy Tadalafil 5mg
Generic Tadalafil 20mg price Cialis over the counter VeritasCare
http://veritascarepharm.com/# cialis for sale
https://corebluehealth.shop/# Viagra generic over the counter
VeritasCare: VeritasCare – п»їcialis generic
CoreBlue Health: CoreBlue Health – sildenafil 50 mg price
VeritasCare VeritasCare buy cialis pill
VeritasCare: Buy Tadalafil 20mg – Buy Cialis online
viagra canadian pharmacy: CivicMeds – best canadian pharmacy online
mexican pharmacy CivicMeds best canadian pharmacy
http://civicmeds.com/# canadian pharmacy cialis reviews
http://veritascarepharm.com/# Generic Cialis without a doctor prescription
cheapest cialis: Generic Tadalafil 20mg price – VeritasCare
cheap canadian pharmacy online: canadian pharmacy without prescription – reputable online pharmacy reddit
Cheapest Sildenafil online CoreBlue Health CoreBlue Health
https://corebluehealth.shop/# CoreBlue Health
california pharmacy: CivicMeds – brazilian pharmacy online
CoreBlue Health: CoreBlue Health – Cheap generic Viagra online
Cialis without a doctor prescription Cialis 20mg price Tadalafil price
VeritasCare: VeritasCare – VeritasCare
https://civicmeds.shop/# canada drug pharmacy
Buy Cialis online Cheap Cialis VeritasCare
VeritasCare: buy cialis pill – Buy Tadalafil 10mg
https://veritascarepharm.com/# VeritasCare
CoreBlue Health: Sildenafil Citrate Tablets 100mg – CoreBlue Health
canada pharmacy online generic pharmacy online best canadian pharmacy to order from
canadian pharmacy levitra: CivicMeds – canadian pharmacy cialis 20mg
VeritasCare: Buy Tadalafil 10mg – VeritasCare
http://corebluehealth.com/# order viagra
discount pharmacy pharmacy discount coupons usa pharmacy
all in one pharmacy: canadian pharmacy price checker – online pharmacy delivery usa
https://corebluehealth.shop/# CoreBlue Health
VeritasCare: cialis for sale – cialis for sale
VeritasCare cheapest cialis VeritasCare
VeritasCare: Cheap Cialis – cialis for sale
http://civicmeds.com/# best australian online pharmacy
Buy Tadalafil 10mg: VeritasCare – Buy Cialis online
CoreBlue Health CoreBlue Health CoreBlue Health
VeritasCare: VeritasCare – Buy Tadalafil 5mg
https://corebluehealth.shop/# Order Viagra 50 mg online
online pharmacy no presc uk: cheapest pharmacy for prescriptions – no rx needed pharmacy
VeritasCare Tadalafil Tablet VeritasCare
Buy Tadalafil 5mg: Buy Tadalafil 20mg – Tadalafil Tablet
Cialis 20mg price: Cialis over the counter – Cialis over the counter
no rx needed pharmacy CivicMeds online pharmacy worldwide shipping
canada drugs online reviews: CivicMeds – online pharmacy group
https://veritascarepharm.com/# VeritasCare
VeritasCare Generic Tadalafil 20mg price VeritasCare
sildenafil online: CoreBlue Health – CoreBlue Health
CoreBlue Health: best price for viagra 100mg – CoreBlue Health
VeritasCare VeritasCare Cialis 20mg price in USA
CoreBlue Health: Viagra generic over the counter – CoreBlue Health
canadian pharmacy meds: CivicMeds – canadian pharmacy india
Cialis 20mg price VeritasCare VeritasCare
foreign online pharmacy: online pharmacy in turkey – canadian pharmacy viagra 50 mg
bitcoin pharmacy online: california pharmacy – ez pharmacy
https://veritascarepharm.com/# VeritasCare
online pharmacy prescription CivicMeds canadian pharmacy meds
best price for viagra 100mg: best price for viagra 100mg – Viagra without a doctor prescription Canada
reputable online pharmacy no prescription CivicMeds canadian pharmacy for viagra
safe canadian pharmacy: cheapest online pharmacy india – canadian pharmacy world coupon
https://corebluehealth.shop/# Viagra tablet online
canadian pharmacy com canadian pharmacy price checker canadian pharmacy prices
http://corebluehealth.com/# Viagra generic over the counter
Cheap generic Viagra online CoreBlue Health best price for viagra 100mg
canadian neighbor pharmacy trustworthy canadian pharmacy canadian drug pharmacy
https://civicmeds.shop/# best canadian pharmacy
VeritasCare VeritasCare Cialis 20mg price in USA
https://corebluehealth.com/# CoreBlue Health
CoreBlue Health CoreBlue Health CoreBlue Health
https://veritascarepharm.com/# Buy Tadalafil 20mg
CoreBlue Health sildenafil over the counter Viagra generic over the counter
https://veritascarepharm.shop/# VeritasCare
CoreBlue Health CoreBlue Health CoreBlue Health
canada drug pharmacy CivicMeds reliable online pharmacy
https://civicmeds.com/# web pharmacy
https://veritascarepharm.com/# VeritasCare
discount pharmacy mexico usa pharmacy canada pharmacy online legit
Cheapest Sildenafil online: Buy Viagra online cheap – sildenafil over the counter
https://corebluehealth.com/# Generic Viagra for sale
VeritasCare Buy Cialis online Buy Tadalafil 10mg
what’s the best online pharmacy: legal online pharmacy coupon code – legitimate canadian pharmacies
cheapest viagra Cheap generic Viagra viagra canada
Cialis without a doctor prescription: Tadalafil Tablet – VeritasCare
https://veritascarepharm.com/# VeritasCare
CoreBlue Health CoreBlue Health Cheap generic Viagra online
canadian pharmacy cialis reviews: CivicMeds – mail order pharmacy
http://civicmeds.com/# canadian drugs pharmacy
Viagra Tablet price CoreBlue Health CoreBlue Health
https://veritascarepharm.com/# Tadalafil Tablet
best rx pharmacy online: the peoples pharmacy – canadian pharmacy online cialis
best price for viagra 100mg best price for viagra 100mg Generic Viagra for sale
reputable canadian online pharmacy: CivicMeds – reputable indian online pharmacy
http://civicmeds.com/# online pharmacy europe
VeritasCare Buy Tadalafil 20mg Cialis without a doctor prescription
CoreBlue Health: order viagra – sildenafil 50 mg price
https://civicmeds.com/# canadian pharmacy ltd
pharmacy online 365 canadian pharmacy viagra reviews top online pharmacy india
indian pharmacy: CivicMeds – best canadian pharmacy for cialis
http://corebluehealth.com/# best price for viagra 100mg
https://pinupazz.top/ pin up
https://pinupazz.top/ pin-up oyunu
https://pin-up-kz.space/ пин ап казино kz
pin up az online pin up
pin up az online pin up
пин ап пин ап кз
https://pinupazz.top/ pin up
pin up az online pin up
https://pin-up-kz.space/ пин ап казино
https://pinupazz.top/ pin up casino
пин ап пин ап казино
pin up pin up
https://pinupaz.online/ pin up az
https://pin-up-kz.space/ пин ап казахстан
https://pinupazz.top/ pin up casino
pin-up pin up
пин ап пин ап кз
pin up pin-up oyunu
https://pin-up-kz.space/ пин ап казино kz
pin up pin up az
pin up az online pin up casino
pin up pin up
пин ап пин ап казино kz
legal online pharmacies in the us: cheapest online pharmacy india – trustworthy online pharmacy
online pharmacy without prescription: online pharmacy india – trusted online pharmacy
https://formulinepharmacy.shop/# trusted online pharmacy
online pharmacy no rx: FormuLine Pharmacy – online pharmacy discount code
medstore online pharmacy: FormuLine Pharmacy – trustworthy online pharmacy
https://accessbridgepharmacy.shop/# AccessBridge Pharmacy
online pharmacy discount code FormuLine Pharmacy trustworthy online pharmacy
SteadyMeds pharmacy: SteadyMeds pharmacy – canadian pharmacy antibiotics
https://steadymedspharmacy.com/# SteadyMeds pharmacy
SteadyMeds: SteadyMeds – SteadyMeds
international pharmacy: top 10 online pharmacy in india – overseas pharmacy no prescription
https://formulinepharmacy.com/# no prescription needed pharmacy
new pharmacy online: reputable indian online pharmacy – п»їinternational drug mart
real canadian pharmacy: SteadyMeds pharmacy – SteadyMeds
AccessBridge Pharmacy mail order pharmacy mexico AccessBridge Pharmacy
http://accessbridgepharmacy.com/# AccessBridge
medstore online pharmacy: FormuLine Pharmacy – us pharmacy no prescription
SteadyMeds: SteadyMeds pharmacy – SteadyMeds pharmacy
https://steadymedspharmacy.com/# canada ed drugs
https://steadymedspharmacy.com/# SteadyMeds pharmacy
AccessBridge Pharmacy: AccessBridge Pharmacy – pharma mexicana
https://accessbridgepharmacy.shop/# AccessBridge
canadian pharmacy online ship to usa: SteadyMeds – canadapharmacyonline
pharmacy order online: FormuLine Pharmacy – safe online pharmacies
https://accessbridgepharmacy.shop/# AccessBridge Pharmacy
https://formulinepharmacy.com/# pharmacy online
AccessBridge: buying prescription drugs in mexico – AccessBridge Pharmacy
canada drugs online: SteadyMeds – canadian pharmacy 24h com
https://accessbridgepharmacy.com/# AccessBridge Pharmacy
top-rated online pharmacies FormuLine Pharmacy online pharmacies
AccessBridge Pharmacy: AccessBridge Pharmacy – AccessBridge
http://formulinepharmacy.com/# us pharmacy no prescription
https://steadymedspharmacy.com/# SteadyMeds pharmacy
AccessBridge: mexican pharmacy what to buy – AccessBridge Pharmacy
online pharmacy no prescription needed: FormuLine Pharmacy – medicine online order
AccessBridge: AccessBridge Pharmacy – online pharmacy in mexico
mexican rx pharm: AccessBridge Pharmacy – AccessBridge Pharmacy
http://formulinepharmacy.com/# reputable overseas online pharmacies
reputable overseas online pharmacies india pharmacy worldwide pharmacy online
Video’s voor volwassenen kunnen worden gestreamd op betrouwbare platforms voor
privacy. Ontdek betrouwbare adult hubs voor kwaliteitsweergave.
Here is my site :: BUY CONCERTA ONLINE
77 canadian pharmacy: rate canadian pharmacies – SteadyMeds
http://accessbridgepharmacy.com/# AccessBridge Pharmacy
trustworthy online pharmacy: top online pharmacy india – us pharmacy no prescription
farmacia pharmacy mexico purchase online: AccessBridge Pharmacy – progreso mexico pharmacy online
https://steadymedspharmacy.com/# SteadyMeds pharmacy
SteadyMeds legal to buy prescription drugs from canada canadian pharmacy 365
https://steadymedspharmacy.com/# canadian pharmacies that deliver to the us
online pharmacy without scripts: FormuLine Pharmacy – best online pharmacy
AccessBridge Pharmacy: AccessBridge – AccessBridge Pharmacy
http://accessbridgepharmacy.com/# AccessBridge
SteadyMeds pharmacy: SteadyMeds – SteadyMeds
https://accessbridgepharmacy.com/# AccessBridge Pharmacy
AccessBridge: AccessBridge – mexican farmacia
medicine online order: online shopping pharmacy india – online pharmacy without scripts
http://formulinepharmacy.com/# reputable online pharmacy no prescription
SteadyMeds pharmacy safe reliable canadian pharmacy SteadyMeds
https://formulinepharmacy.com/# buy drugs online
new pharmacy online: FormuLine Pharmacy – best online pharmacy no prescription
AccessBridge Pharmacy: AccessBridge – mexican online mail order pharmacy
https://steadymedspharmacy.shop/# certified canadian pharmacy
AccessBridge: purple pharmacy online – AccessBridge Pharmacy
https://accessbridgepharmacy.com/# AccessBridge Pharmacy
ordering drugs from canada canadianpharmacymeds SteadyMeds
the canadian pharmacy: SteadyMeds – adderall canadian pharmacy
http://steadymedspharmacy.com/# SteadyMeds pharmacy
us pharmacy no prescription: Online medicine home delivery – express scripts mail order pharmacy
http://formulinepharmacy.com/# online pharmacy no rx
AccessBridge Pharmacy: AccessBridge – mexico meds
best rx pharmacy online: FormuLine Pharmacy – legit online pharmacy
http://accessbridgepharmacy.com/# AccessBridge Pharmacy
SteadyMeds: legitimate canadian online pharmacies – pharmacy rx world canada
Beste pornosites bieden hoogwaardige inhoud voor volwassen entertainment.
Kies voor betrouwbare hubs voor een veilige en plezierige ervaring.
Also visit my site – buy Concerta online
SteadyMeds pharmacy canadian pharmacies canada pharmacy online
https://accessbridgepharmacy.shop/# AccessBridge Pharmacy
SteadyMeds pharmacy: safe canadian pharmacies – trusted canadian pharmacy
SteadyMeds pharmacy: SteadyMeds – SteadyMeds pharmacy
https://accessbridgepharmacy.shop/# AccessBridge
mexico medicine: AccessBridge – medication from mexico
AccessBridge: AccessBridge – mexican pharmacy near me
online erectile dysfunction prescription: cheap ed medication – express scripts mail order pharmacy
http://petcanadadirect.com/# Pet Canada Direct
buy drugs online: Pharm Rate – buy online medicine
Pharm Rate: Pharm Rate – Pharm Rate
Pharm Rate online pharmacy Pharm Rate
http://pharmrate.com/# reputable overseas online pharmacies
pet med: Pet Canada Direct – Pet Canada Direct
cheapest ed online: low cost ed meds – medstore online pharmacy
http://edmedscoupon.com/# edmeds
vet pharmacy: pet prescriptions online – canada pet meds
Pharm Rate: online pharmacy no rx – Pharm Rate
international pharmacy no prescription pharmacy paypal Pharm Rate
https://pharmrate.com/# Pharm Rate
Pet Canada Direct: Pet Canada Direct – п»їdog medication online
Pet Canada Direct: vet pharmacy – Pet Canada Direct
https://pharmrate.com/# п»їinternational drug mart
Pet Canada Direct: Pet Canada Direct – pet meds for dogs
order ed pills online: best ed pills online – safe online pharmacies
Pet Canada Direct pet med canada pet meds
Pharm Rate: worldwide pharmacy – Pharm Rate
https://petcanadadirect.com/# pet pharmacy
cheapest ed online: cheap ed – medicine online
ed pills cheap pills for erectile dysfunction online reputable online pharmacy no prescription
Pet Canada Direct: п»їdog medication online – Pet Canada Direct
http://edmedscoupon.com/# where can i get ed pills
online ed pharmacy: Ed Meds Coupon – top-rated online pharmacies
online pet pharmacy: pet prescriptions online – vet pharmacy online
http://petcanadadirect.com/# п»їdog medication online
cheapest ed meds: Ed Meds Coupon – trusted online pharmacy
antibiotics online prescription antibiotics cheap buy antibiotics for uti
is wegovy the same as semaglutide: semaglutide life – online pharmacy no rx
https://semaglutide.life/# how to get insurance to cover rybelsus
rybelsus cost in mexico: semaglutide life – reputable overseas online pharmacies
rybelsus how to get: doses of rybelsus – best online pharmacy no prescription
https://antibiotics.cheap/# over the counter antibiotics
compounded semaglutide left out of fridge semaglutide life rybelsus 7 mg oral tablet
stromectol reviews: stromectol reviews – stromectol uk buy
stromectol reviews: stromectol reviews – ivermectin iv
https://antibiotics.cheap/# antibiotics
rybelsus compounding pharmacy: semaglutide life – new pharmacy online
https://antibiotics.cheap/# over the counter antibiotics
over the counter antibiotics: antibiotics cheap – online antibiotics
over the counter antibiotics over the counter antibiotics antibiotics for uti
buy antibiotics online: over the counter antibiotics – antibiotics cheap
https://semaglutide.life/# how long does it take for semaglutide to get out of your system
antibiotics over the counter: over the counter antibiotics – generic antibiotics online pharmacy
semaglutide vs compounded semaglutide: does rybelsus cause headaches – no rx needed pharmacy
https://antibiotics.cheap/# antibiotics cheap
stromectol reviews: stromectol reviews – stromectol usa
stromectol reviews stromectol how much it cost stromectol reviews
https://stromectol.reviews/# ivermectin cost canada
ivermectin otc: stromectol reviews – stromectol reviews
https://stromectol.reviews/# stromectol reviews
is semaglutide safe for weight loss: farxiga and rybelsus together – no prescription needed pharmacy
generic antibiotics online pharmacy over the counter antibiotics buy antibiotics for uti
ivermectin usa price: stromectol – stromectol reviews
https://antibiotics.cheap/# antibiotics cheap
semaglutide vs phentermine: how many mg is 10 units of semaglutide – top online pharmacy
weight watchers semaglutide reviews: semaglutide life – shop medicine online
https://antibiotics.cheap/# buy antibiotics from india
rybelsus to ozempic conversion: oral semaglutide weight loss reviews – reliable online pharmacy
https://shorturl.fm/IPl9r
novo rybelsus: semaglutide life – express scripts mail order pharmacy
rybelsus vs wegovy for weight loss semaglutide life what is the starting dose of semaglutide
https://antibiotics.cheap/# antibiotic without presription
ivermectin pills canada: stromectol reviews – stromectol reviews
ivermectin 500mg: stromectol reviews – stromectol reviews
https://antibiotics.cheap/# antibiotics cheap
otc antibiotics: antibiotics cheap – over the counter antibiotics
semaglutide dosing for weight loss: rybelsus vs ozempic vs wegovy – online drugs order
stromectol reviews ivermectin pill cost ivermectin 1
https://stromectol.reviews/# stromectol 3mg cost
rybelsus tablet: semaglutide life – international pharmacy
ivermectin iv: where to buy ivermectin pills – stromectol reviews
https://stromectol.reviews/# stromectol reviews
can you buy antibiotics over the counter: antibiotics for uti over the counter – cheapest antibiotics
stromectol reviews: ivermectin usa price – ivermectin australia
over the counter antibiotics buy amoxicillin over the counter antibiotics
https://stromectol.reviews/# ivermectin 3 mg tabs
ozempic o rybelsus para adelgazar: semaglutide life – best mail order pharmacy
stromectol reviews: stromectol reviews – stromectol reviews
https://antibiotics.cheap/# antibiotics cheap
antibiotics cheap: antibiotics cheap – cheapest antibiotics
long term effects of rybelsus: semaglutide and birth control – online pharmacy discount code
https://antibiotics.cheap/# over the counter antibiotics
rybelsus medication class rybelsus oral rybelsus 14 mg
stromectol 3 mg tablet: stromectol ivermectin – stromectol reviews
over the counter antibiotics: over the counter antibiotics – over the counter antibiotics
https://stromectol.reviews/# ivermectin cream 1%
rybelsus bottle: semaglutide units to mg – pharmacy order online
how many mg is 10 units of semaglutide: semaglutide life – worldwide pharmacy
https://antibiotics.cheap/# otc antibiotics
stromectol reviews stromectol reviews purchase ivermectin
generic ivermectin for humans: stromectol reviews – stromectol reviews
buy antibiotics for uti: over the counter antibiotics – can you buy antibiotics over the counter
https://antibiotics.cheap/# generic antibiotics
side effects of rybelsus 3 mg tablet: semaglutide life – top-rated online pharmacies
goodrx semaglutide: semaglutide life – pharmacy online
https://semaglutide.life/# semaglutide calculator
is ozempic or rybelsus better for weight loss: semaglutide pros and cons – secure medical online pharmacy
how much is rybelsus semaglutide stomach pain how long does it take for semaglutide to work
antibiotics cheap: over the counter antibiotics – antibiotics cheap
https://stromectol.reviews/# ivermectin canada
stromectol reviews: stromectol reviews – stromectol reviews
Canadian Tabs: Canadian Tabs – canada drugstore pharmacy rx
https://canadiantabs.xyz/# canada drugs online reviews
Canadian Tabs: Canadian Tabs – www canadianonlinepharmacy
world pharmacy india cheapest online pharmacy india overseas online pharmacy
world pharmacy india: world pharmacy india – trustworthy online pharmacy
http://canadiantabs.com/# Canadian Tabs
reputable indian pharmacies: top 10 pharmacies in india – shop medicine online
canadian pharmacy cheap: canadian pharmacy king reviews – Canadian Tabs
https://indianmedsdelivery.com/# indianpharmacy com
indian pharmacy: reputable indian online pharmacy – medicine online order
Canadian Tabs Canadian Tabs pharmacy rx world canada
canadapharmacyonline com: Canadian Tabs – canadian pharmacies
http://canadiantabs.com/# Canadian Tabs
Canadian Tabs: pharmacy canadian – Canadian Tabs
indian pharmacy: indianpharmacy com – international pharmacy
https://mexicanpharm.com/# buying prescription drugs in mexico
Mexican Pharm: Mexican Pharm – mexican online mail order pharmacy
Mexican Pharm can i order online from a mexican pharmacy mexi pharmacy
top online pharmacy india: Indian Meds Delivery – online pharmacy without prescription
http://canadiantabs.com/# Canadian Tabs
top 10 online pharmacy in india: Indian Meds Delivery – online pharmacy no rx
https://mexicanpharm.xyz/# mexico pharmacy order online
vipps approved canadian online pharmacy: canadian mail order pharmacy – thecanadianpharmacy
canada drug pharmacy: Canadian Tabs – canadian drug pharmacy
best mexican online pharmacy online drugs order mexican pharmacies that ship
https://indianmedsdelivery.xyz/# Online medicine order
Mexican Pharm: mexico online pharmacy – Mexican Pharm
Mexican Pharm: Mexican Pharm – Mexican Pharm
https://mexicanpharm.xyz/# mexican medicine store
best mexican pharmacy: Mexican Pharm – tijuana pharmacy online
mexican rx: best pharmacy in mexico – order medication from mexico
canadian pharmacies Canadian Tabs canada pharmacy online legit
http://mexicanpharm.com/# Mexican Pharm
affordable pharmacy: purple pharmacy – meds from mexico
india pharmacy mail order: cheapest online pharmacy india – international pharmacy
pharmacy website india: Indian Meds Delivery – best mail order pharmacy
canada pharmacy online: Canadian Tabs – canadian pharmacy tampa
canadian drug stores canadian pharmacy meds Canadian Tabs
http://canadiantabs.com/# Canadian Tabs
Canadian Tabs: Canadian Tabs – canadian pharmacy reviews
п»їcanadian pharmacy uk delivery: canada cloud pharmacy – canadian pharmacy world
https://onlinepharmfirst.com/# worldwide pharmacy
trustworthy online pharmacy: Online Pharm First – top-rated online pharmacies
Ivermectin First: stromectol prices – Ivermectin First
Ivermectin First stromectol 3 mg tablet Ivermectin First
https://ivermectinfirst.shop/# ivermectin cream
Ivermectin First: Ivermectin First – Ivermectin First
stromectol nz: Ivermectin First – Ivermectin First
http://onlinepharmfirst.com/# no prescription pharmacy paypal
no prescription needed pharmacy: worldwide pharmacy – new pharmacy online
reputable overseas online pharmacies: pharmacy order online – online pharmacy no prescription needed
stromectol nz Ivermectin First Ivermectin First
https://ivermectinfirst.shop/# Ivermectin First
Ivermectin First: Ivermectin First – ivermectin 4
pet meds for dogs: vet pharmacy online – Vet Pharm First
http://ivermectinfirst.com/# Ivermectin First
pet prescriptions online: dog prescriptions online – Vet Pharm First
ivermectin cream 1%: stromectol tablets – ivermectin 8 mg
https://ivermectinfirst.shop/# ivermectin over the counter canada
Ivermectin First Ivermectin First Ivermectin First
worldwide pharmacy online: Online Pharm First – worldwide pharmacy
https://onlinepharmfirst.com/# п»їinternational drug mart
pet meds official website: Vet Pharm First – vet pharmacy online
https://onlinepharmfirst.shop/# us pharmacy no prescription
ivermectin oral solution: ivermectin 3 – ivermectin iv
legal online pharmacies in the us: no prescription pharmacy paypal – buy online medicine
Vet Pharm First Vet Pharm First best pet rx
https://onlinepharmfirst.shop/# online drugs order
cost of ivermectin medicine: Ivermectin First – Ivermectin First
http://onlinepharmfirst.com/# medicine online
best mail order pharmacy: Online Pharm First – no rx needed pharmacy
п»їdog medication online: pet pharmacy online – Vet Pharm First
https://onlinepharmfirst.com/# top online pharmacy
pharmacy websites: Online Pharm First – no prescription needed pharmacy
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
worldwide pharmacy online Online Pharm First best online pharmacy
https://vetpharmfirst.com/# pet med
Vet Pharm First: Vet Pharm First – Vet Pharm First
https://vetpharmfirst.com/# Vet Pharm First
Ivermectin First: Ivermectin First – Ivermectin First
https://ivermectinfirst.com/# Ivermectin First
pet prescriptions online: canada pet meds – vet pharmacy online
Vet Pharm First Vet Pharm First dog prescriptions online
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://www.binance.info/register?ref=JW3W4Y3A
https://onlinepharmfirst.com/# reputable overseas online pharmacies
worldwide pharmacy: legitimate online pharmacy – pharmacy online
https://onlinepharmfirst.com/# online pharmacy without scripts
best mail order pharmacy: no prescription pharmacy paypal – overseas online pharmacy
https://vetpharmfirst.shop/# dog prescriptions online
ivermectin 5 mg: Ivermectin First – Ivermectin First
ivermectin usa price Ivermectin First stromectol tablets uk
https://ivermectinfirst.com/# ivermectin lotion cost
Ivermectin First: ivermectin 4 – stromectol australia
https://vetpharmfirst.com/# pet pharmacy
pharmacy no prescription required: Online Pharm First – best rx pharmacy online
https://onlinepharmfirst.com/# best online pharmacy no prescription
legal online pharmacy Online Pharm First express scripts mail order pharmacy
https://cialis.sbs/# cheapest cialis
cialis for sale Generic Tadalafil 20mg price cialis for sale
https://viagra.onl/# Generic Viagra online
https://viagra.onl/# buy viagra here
does rybelsus have cardiovascular benefits what does rybelsus do buy online medicine
Cialis over the counter Generic Cialis without a doctor prescription Buy Tadalafil 10mg
https://cialis.sbs/# Buy Cialis online
https://viagra.onl/# sildenafil 50 mg price
sildenafil over the counter generic sildenafil sildenafil over the counter
https://rybelsus.pro/# highest dose of semaglutide
https://rybelsus.pro/# does semaglutide have to be refrigerated
half life of rybelsus diabetes medications rybelsus medicine online
Cheap Viagra 100mg buy Viagra online Viagra Tablet price
https://rybelsus.pro/# rybelsus active ingredient
https://cialis.sbs/# Generic Cialis without a doctor prescription
semaglutide diarrhea treatment how often do you take semaglutide new pharmacy online
cialis for sale Cialis 20mg price in USA Cialis 20mg price in USA
https://rybelsus.pro/# rybelsus gas
https://rybelsus.pro/# 40 units of semaglutide is how many ml
Order Viagra 50 mg online Viagra tablet online Buy generic 100mg Viagra online
п»їcialis generic Buy Tadalafil 10mg Buy Tadalafil 20mg
https://viagra.onl/# Sildenafil 100mg price
https://cialis.sbs/# cheapest cialis
Buy Tadalafil 10mg Tadalafil Tablet Generic Cialis without a doctor prescription
https://cialis.sbs/# Generic Cialis without a doctor prescription
14 mg rybelsus to mounjaro rybelsus cost goodrx rybelsus long term side effects
https://cialis.sbs/# cialis for sale
Cialis 20mg price buy cialis pill Buy Cialis online
https://cialis.sbs/# buy cialis pill
Tadalafil Tablet Buy Tadalafil 10mg Cialis without a doctor prescription
https://cialis.sbs/# Cialis without a doctor prescription
https://viagra.onl/# Viagra online price
does semaglutide cause cancer why am i gaining weight on semaglutide weight loss rybelsus
can you take rybelsus and metformin together rybelsus approval date medstore online pharmacy
https://viagra.onl/# buy Viagra online
https://cialis.sbs/# Tadalafil price
fda semaglutide shortage compound semaglutide reputable online pharmacy no prescription
https://viagra.onl/# Cheap generic Viagra online
https://viagra.onl/# over the counter sildenafil
cheap viagra Sildenafil 100mg price buy viagra here
Cheap generic Viagra Viagra tablet online Cheap Sildenafil 100mg
https://viagra.onl/# over the counter sildenafil
https://rybelsus.pro/# rybelsus buy online
rybelsus pill form order rybelsus online overseas online pharmacy
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
https://cialis.sbs/# Buy Tadalafil 10mg
Buy Cialis online buy cialis pill Cialis without a doctor prescription
https://rybelsus.pro/# rybelsus precio en walmart
https://viagra.onl/# Cheap generic Viagra
benefits of rybelsus semaglutide shots rybelsus daily
is compounded semaglutide the same as ozempic does rybelsus cause fatigue online pharmacy
https://cialis.sbs/# cialis for sale
https://rybelsus.pro/# does compounded semaglutide work
semaglutide vomiting semaglutide compound side effects online pharmacy discount code
https://rybelsus.pro/# rybelsus tablets
cheapest viagra Cheap Sildenafil 100mg best price for viagra 100mg
https://bestbetgiris.online# pusulabet giris
https://casivipgiris.site# bahiscasino güncel
bahiscasino bahiscasino giris
bahiscasino: bahiscasino resmi
pusulabet casino pusulabet resmi giriş
bahiscasino güncel adres: bahiscasino güncel adres
bahiscasino güncel adres: bahiscasino resmi giriş
semaglutide depression reviews on rybelsus how to give yourself a shot of semaglutide
pusulabet giris: pusulabet güncel adres
indian pharmacy paypal: mail order pharmacy india – online drugs order
indian pharmacy online Easy India Meds legit online pharmacy
best mexican online pharmacy: Easy Mex Meds – mexican farmacia
mexicanrxpharm Easy Mex Meds hydrocodone mexico pharmacy
Easy Mex Meds: Easy Mex Meds – progreso, mexico pharmacy online
Easy Canada Meds: Easy Canada Meds – Easy Canada Meds
http://easyindiameds.com/# Online medicine home delivery
indian pharmacy paypal reputable indian pharmacies no rx needed pharmacy
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
mexican pharmacy online medications: Easy Mex Meds – mexico rx
Easy Mex Meds mexico meds Easy Mex Meds
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
https://easyindiameds.com/# indian pharmacy
indianpharmacy com: cheapest online pharmacy india – no prescription needed pharmacy
canadian drug stores Easy Canada Meds Easy Canada Meds
Easy Canada Meds: canadian pharmacies – Easy Canada Meds
Adult videos can be streamed on trusted platforms for privacy.
Explore safe websites for quality viewing.
my page Buy Rivotril
mexican online mail order pharmacy: mexican pharmacies – Easy Mex Meds
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
Easy Mex Meds Easy Mex Meds online mexico pharmacy
https://easymexmeds.shop/# Easy Mex Meds
Easy Mex Meds: farmacia pharmacy mexico purchase online – Easy Mex Meds
indian pharmacy online: indian pharmacy online – online pharmacy no prescription needed
online shopping pharmacy india reputable indian pharmacies best rx pharmacy online
Seksuele inhoud is breed beschikbaar op speciale platforms voor volwassenen. Kies
voor veilige sites voor veiligheid.
Also visit my page buy cialis online
pharmacy canadian superstore: Easy Canada Meds – best canadian pharmacy to buy from
Easy Mex Meds mexican pharmacy las vegas mexico pharmacy list
best online pharmacy india: reputable indian pharmacies – medstore online pharmacy
Easy Canada Meds: Easy Canada Meds – legal canadian pharmacy online
buy medicines online in india Easy India Meds medicine online
http://easycanadameds.com/# Easy Canada Meds
best canadian pharmacy online: legitimate canadian pharmacies – buy prescription drugs from canada cheap
Easy Mex Meds: order medicine from mexico – Easy Mex Meds
pharmacy com canada Easy Canada Meds canadian pharmacy scam
View explicit material safely by choosing verified adult websites.
Opt for secure platforms for discreet entertainment.
Check out my blog BUY RITALIN ONLINE
Easy Canada Meds: canadian pharmacy – onlinecanadianpharmacy 24
Easy Mex Meds: mexican meds – mexican rx
farmacia mexicana en linea Easy Mex Meds farmacia mexicana en linea
http://easycanadameds.com/# Easy Canada Meds
Easy Canada Meds: canada drugs online reviews – Easy Canada Meds
Easy Mex Meds mexico medication Easy Mex Meds
Easy Canada Meds: Easy Canada Meds – canadian pharmacy 1 internet online drugstore
Easy Canada Meds: my canadian pharmacy – Easy Canada Meds
mail order pharmacy india Easy India Meds legal online pharmacy
Expliciete webplatform biedt een reeks video’s voor adult entertainment.
Kies voor gegarandeerde porno hubs voor een veilige ervaring.
reputable indian pharmacies: cheapest online pharmacy india – best mail order pharmacy
mexican pharmacies that ship to us Easy Mex Meds mexico pharmacy list
india pharmacy mail order: Easy India Meds – п»їinternational drug mart
canadian pharmacy no rx needed: Easy Canada Meds – Easy Canada Meds
https://easyindiameds.shop/# buy prescription drugs from india
best canadian online pharmacy canadian drugs pharmacy the canadian pharmacy
Easy Canada Meds: trustworthy canadian pharmacy – Easy Canada Meds
cheapest online pharmacy india: indianpharmacy com – online pharmacy without scripts
Sex is widely available on dedicated platforms for mature audiences.
Opt for trusted adult hubs to ensure safety.
my blog: Buy Rivotril
Easy Mex Meds mexico meds Easy Mex Meds
Easy Canada Meds: Easy Canada Meds – Easy Canada Meds
Easy Canada Meds: Easy Canada Meds – pharmstore canada
reputable indian pharmacies Easy India Meds п»їinternational drug mart
buy prescription drugs from india: Easy India Meds – express scripts mail order pharmacy
п»їlegitimate online pharmacies india: Easy India Meds – legal online pharmacies in the us
http://easymexmeds.com/# mexican medicine store
Easy Canada Meds Easy Canada Meds canadian pharmacies that deliver to the us
canadian pharmacy meds: canadian pharmacy victoza – legit canadian pharmacy
order meds from mexico: Easy Mex Meds – Easy Mex Meds
Easy Mex Meds Easy Mex Meds medicine mexico
Online medicine home delivery: india pharmacy mail order – buy online medicine
online canadian pharmacy reviews: Easy Canada Meds – canadian pharmacy drugs online
india online pharmacy Easy India Meds top online pharmacy
buy prescription drugs from india: Easy India Meds – overseas online pharmacy
https://easymexmeds.com/# Easy Mex Meds
Easy Mex Meds: worldwide pharmacy – Easy Mex Meds
mexican drugstore Easy Mex Meds pharmacies in mexico
reputable indian online pharmacy: indianpharmacy com – legit online pharmacy
good online mexican pharmacy: order medicine from mexico – pharmacia mexico
indian pharmacy online Easy India Meds best online pharmacy
mexico drug store online: Easy Mex Meds – medicine from mexico
Easy Canada Meds canadian pharmacy sarasota legitimate canadian online pharmacies
mexican meds: Easy Mex Meds – Easy Mex Meds
mail order pharmacy india: Easy India Meds – worldwide pharmacy online
https://easyindiameds.shop/# world pharmacy india
canadian pharmacy drugs online Easy Canada Meds the canadian drugstore
Easy Canada Meds: best canadian pharmacy – canadian neighbor pharmacy
Easy Canada Meds: Easy Canada Meds – canada pharmacy online website shopping
cheapest online pharmacy india best india pharmacy buy drugs online
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
https://easyindiameds.shop/# best online pharmacy india
reputable canadian online pharmacy: canadian pharmacy world reviews – Easy Canada Meds
Easy Mex Meds pharmacia mexico Easy Mex Meds
п»їmexican pharmacy: Easy Mex Meds – can i buy meds from mexico online
canadian drugstore online: Easy Canada Meds – Easy Canada Meds
india pharmacy mail order Online medicine home delivery shop medicine online
Easy Canada Meds: canadian pharmacy victoza – buying from canadian pharmacies
world pharmacy india: Easy India Meds – no prescription pharmacy paypal
best canadian pharmacy online Easy Canada Meds canadian drug prices
http://easycanadameds.com/# Easy Canada Meds
mexican pharmacy near me: mexico pharmacy list – is mexipharmacy legit
online mexican pharmacies: mexican pharmacies online drugs – best mexican online pharmacy
Easy Mex Meds reputable mexican pharmacy mexican pharmacy ship to usa
can i order online from a mexican pharmacy: pharmacy mexico online – best mexican pharmacy
world pharmacy india: Easy India Meds – buy drugs online
mail order pharmacy india indian pharmacy no prescription pharmacy paypal
https://easyindiameds.com/# cheapest online pharmacy india
Easy Canada Meds: Easy Canada Meds – Easy Canada Meds
canadian pharmacy no scripts: canada pharmacy – Easy Canada Meds
Easy Mex Meds Easy Mex Meds Easy Mex Meds
https://freshpharm24.com/product/norvasc express scripts mail order pharmacy
pharmacy worldwide pharmacy
Fresh Pharm 24 us pharmacy no prescription
https://freshpharm24.com/ foreign online pharmacy
Fresh Pharm 24 online pharmacy discount code
https://freshpharm24.com/ foreign online pharmacy
https://freshpharm24.com/product/stendra new pharmacy online
pharmacy fresh pharm online pharmacy without prescription
Fresh Pharm worldwide pharmacy online
https://freshpharm24.com/product/levothroid buy drugs online
Fresh Pharm 24 foreign online pharmacy
cialis secure medical online pharmacy
https://freshpharm24.com/product/levothroid online drugs order
https://freshpharm24.com/product/lipitor no prescription needed pharmacy
pharmacy trustworthy online pharmacy
generic viagra reputable online pharmacy no prescription
https://freshpharm24.com/product/priligy online pharmacy no prescription
Fresh Pharm 24 online pharmacy without prescription
https://freshpharm24.com/product/cialis trustworthy online pharmacy
https://freshpharm24.com/ foreign online pharmacy
Fresh Pharm foreign online pharmacy
Fresh Pharm 24 medicine online
https://freshpharm24.com/ medicine online order
Fresh Pharm international pharmacy
Fresh Pharm best rx pharmacy online
https://freshpharm24.com/ online pharmacy no prescription needed
lipitor trustworthy online pharmacy
pharmacy fresh pharm worldwide pharmacy
https://freshpharm24.com/product/lipitor buy drugs online
https://freshpharm24.com/ best mail order pharmacy
Fresh Pharm 24 pharmacy order online
Fresh Pharm 24 online pharmacy without scripts
https://freshpharm24.com/product/cialis medicine online
https://cialisvip.online/# Buy Tadalafil 10mg
Sildenafil Citrate Tablets 100mg Sildenafil Vip Order Viagra 50 mg online
Cheap generic Viagra Sildenafil Vip viagra without prescription
http://stromectolvip.com/# ivermectin cream
cheapest viagra over the counter sildenafil Buy generic 100mg Viagra online
https://sildenafilvip.com/# Sildenafil Vip
https://stromectolvip.com/# ivermectin 4 tablets price
Sildenafil Citrate Tablets 100mg Sildenafil Vip sildenafil 50 mg price
https://cialisvip.com/# Cialis Vip
http://stromectolvip.com/# ivermectin iv
ivermectin 200mg stromectol ireland ivermectin lotion for lice
Generic Viagra for sale Sildenafil Vip viagra without prescription
http://stromectolvip.com/# stromectol 3 mg tablet
https://stromectolvip.com/# ivermectin pills canada
Viagra Tablet price cheap viagra Buy generic 100mg Viagra online
https://cialisvip.online/# Cialis Vip
https://cialisvip.com/# Generic Cialis without a doctor prescription
Cialis 20mg price in USA Cialis 20mg price in USA Cheap Cialis
stromectol cream stromectol Vip can you buy stromectol over the counter
https://stromectolvip.com/# ivermectin 12
https://sildenafilvip.com/# Sildenafil Vip
Cheap Cialis Buy Cialis online Buy Tadalafil 10mg
https://sildenafilvip.com/# Sildenafil Vip
https://sildenafilvip.com/# over the counter sildenafil
Buy Tadalafil 10mg Cialis Vip Cheap Cialis
Order Viagra 50 mg online Cheap Viagra 100mg viagra without prescription
https://cialisvip.online/# Cialis Vip
https://stromectolvip.online/# stromectol otc
generic sildenafil Sildenafil Vip Cheap generic Viagra online
http://sildenafilvip.com/# Sildenafil Vip
https://cialisvip.com/# Cialis Vip
Cialis without a doctor prescription Cialis Vip Buy Tadalafil 5mg
https://sildenafilvip.com/# Cheap Sildenafil 100mg
Viagra tablet online order viagra Viagra without a doctor prescription Canada
https://sildenafilvip.shop/# Buy Viagra online cheap
Buy generic 100mg Viagra online Sildenafil Vip best price for viagra 100mg
https://stromectolvip.online/# stromectol 3mg tablets
cialis for sale Buy Tadalafil 20mg Buy Tadalafil 20mg
https://stromectolvip.com/# ivermectin cream cost
Viagra online price Sildenafil Vip cheap viagra
http://sildenafilvip.com/# Sildenafil Vip
Cheap generic Viagra Sildenafil Vip Cheap Viagra 100mg
http://cialisvip.com/# Cialis Vip
Generic Viagra for sale Buy Viagra online cheap Cheapest Sildenafil online
https://sildenafilvip.shop/# Sildenafil Vip
Buy Cialis online Cialis Vip cialis for sale
http://sildenafilvip.com/# Buy generic 100mg Viagra online
Cheap Cialis Tadalafil Tablet Buy Tadalafil 20mg
ivermectin over the counter canada ivermectin usa price ivermectin for sale
http://sildenafilvip.com/# Generic Viagra for sale
cheap viagra Generic Viagra online Order Viagra 50 mg online
https://cialisvip.online/# Cialis Vip
Viagra online price Sildenafil Vip Viagra tablet online
http://cialisvip.com/# Cialis Vip
Tadalafil Tablet cialis for sale Generic Cialis without a doctor prescription
Buy Cialis online Tadalafil price Cheap Cialis
https://sildenafilvip.com/# Cheap generic Viagra
cheap viagra Sildenafil Vip Cheapest Sildenafil online
https://stromectolvip.com/# ivermectin drug
Viagra online price Buy Viagra online cheap cheap viagra
https://cialisvip.com/# Cialis 20mg price in USA
ivermectin 2mg stromectol Vip stromectol in canada
buy ivermectin nz stromectol Vip stromectol price in india
https://stromectolvip.com/# stromectol tablets for humans
liraglutide fast delivery cheap liraglutide cheap victoza
https://victopharm.com/# trustworthy online pharmacy
legal online pharmacy online pharmacies legitimate online pharmacy
cheap liraglutide liraglutide liraglutide fast delivery
http://semaglutideglp1.com/# is zepbound a semaglutide
online pharmacy no prescription no rx needed pharmacy online pharmacy no prescription
liraglutide online LiraglutideGlp1 cheap victoza
http://semaglutideglp1.com/# semaglutide starting dose for weight loss
п»їinternational drug mart Victo Pharm pharmacy no prescription required
generic liraglutide buy victoza glp-1
https://victopharm.shop/# overseas online pharmacy
does semaglutide cause heartburn glp 1 pills rybelsus coupons
legitimate online pharmacy pharmacy no prescription required buy online medicine
https://liraglutideglp1.shop/# liraglutide online
victoza weight loss LiraglutideGlp1 liraglutide online
liraglutide liraglutide price liraglutide pharmacy
https://victopharm.com/# medicine online
half life of rybelsus glp-1 how many units is 1 mg of semaglutide
victoza delivery liraglutide victoza generic
https://liraglutideglp1.com/# liraglutide otc
buy victoza liraglutide online cheap victoza
rybelsus symptoms why is semaglutide not working for me rybelsus 3 mg cost
https://semaglutideglp1.shop/# hers semaglutide cost
cheap victoza cheap liraglutide cheap liraglutide
victoza generic victoza glp 1
https://victopharm.com/# foreign online pharmacy
http://victopharm.com/# pharmacy online
worldwide pharmacy reliable online pharmacy best online pharmacy no prescription
buy victoza LiraglutideGlp1 buy liraglutide online
over the counter sildenafil UroHealth Daily – sildenafil 50 mg price
Viagra online price Cheapest Sildenafil online – buy Viagra over the counter
buy Viagra online UroHealth Daily – Generic Viagra online
Cheapest Sildenafil online best price for viagra 100mg – Generic Viagra for sale
Order Viagra 50 mg online Buy generic 100mg Viagra online – Order Viagra 50 mg online
sildenafil 50 mg price Buy Viagra online cheap viagra canada
Buy Viagra online cheap Viagra without a doctor prescription Canada – buy viagra here
sildenafil online UroHealth Daily – buy Viagra online
viagra without prescription UroHealth Daily – buy viagra here
cheapest viagra Order Viagra 50 mg online – Cheapest Sildenafil online
Viagra online price Sildenafil Citrate Tablets 100mg – Viagra online price
Buy generic 100mg Viagra online Generic Viagra online – Viagra without a doctor prescription Canada
viagra without prescription over the counter sildenafil Order Viagra 50 mg online
Viagra generic over the counter UroHealth Daily – Cheap Viagra 100mg
Cheap generic Viagra Cheap Sildenafil 100mg – Viagra tablet online
Viagra generic over the counter UroHealth Daily – sildenafil over the counter
Cheapest Sildenafil online Viagra tablet online – buy Viagra over the counter
Cheap Viagra 100mg Cheapest Sildenafil online – Order Viagra 50 mg online
Order Viagra 50 mg online Buy Viagra online cheap – Cheap generic Viagra online
Buy generic 100mg Viagra online UroHealth Daily – Viagra generic over the counter
sildenafil over the counter Viagra generic over the counter – sildenafil online
buy Viagra online UroHealth Daily – Cheap generic Viagra online
п»їcialis generic MensRxGuide – Buy Tadalafil 20mg
Cialis 20mg price in USA Tadalafil price – cheapest cialis
http://mensrxguide.org/# Cialis 20mg price in USA
Cialis over the counter Generic Cialis price – Cialis over the counter
Cialis over the counter Tadalafil price – Cialis 20mg price
cheapest cialis Cheap Cialis Tadalafil price
https://mensrxguide.org/# buy cialis pill
Buy Tadalafil 20mg MensRxGuide – Cialis 20mg price
Tadalafil Tablet Buy Tadalafil 5mg – Generic Cialis without a doctor prescription
Buy Tadalafil 5mg Generic Cialis price – Buy Tadalafil 5mg
https://mensrxguide.org/# Generic Cialis price
cialis for sale MensRxGuide – Buy Tadalafil 5mg
Buy Tadalafil 5mg Buy Tadalafil 20mg Cialis 20mg price in USA
Cialis without a doctor prescription Generic Cialis price – Tadalafil Tablet
Generic Cialis price cheapest cialis – Cialis without a doctor prescription
http://mensrxguide.org/# Cialis without a doctor prescription
п»їcialis generic Tadalafil Tablet – Cialis 20mg price in USA
Buy Tadalafil 5mg MensRxGuide – Cialis without a doctor prescription
Buy Cialis online MensRxGuide – Cialis 20mg price in USA
Tadalafil price MensRxGuide – п»їcialis generic
http://mensrxguide.org/# Tadalafil price
Cialis over the counter MensRxGuide – Tadalafil price
п»їcialis generic MensRxGuide – Generic Cialis price
Buy Tadalafil 5mg MensRxGuide – Generic Tadalafil 20mg price
https://mensrxguide.org/# Cialis 20mg price
Cialis 20mg price in USA cheapest cialis – Buy Tadalafil 20mg
AMRI https://usobesityscience.org/tirzepatide-analysis/ semaglutide and birth control
canadian pharmacy rybelsus glp-1 agonists
liraglutide fast delivery Advancing Clinical Research in Metabolic Health and Weight Management
rybelsus mexico tirzepatide
semaglutide https://usobesityscience.org/liraglutide-studies/ rybelsus weight loss uk
rybelsus medicamento tirzepatide
us obesity science https://usobesityscience.org/glp-1-agonists/ generic liraglutide
victoza weight loss liraglutide
Your article helped me a lot, is there any more related content? Thanks!
liraglutide otc AMRI
liraglutide fast delivery orlistat
rybelsus patient assistance AMRI
rybelsus bottle semaglutide
semaglutide https://usobesityscience.org/tirzepatide-analysis/ liraglutide online
adderall and semaglutide liraglutide
victoza delivery orlistat
canadian pharmacy rybelsus Advancing Clinical Research in Metabolic Health and Weight Management
semaglutide https://usobesityscience.org/orlistat-clinical-review/ cheap victoza
rybelsus tablets semaglutide
us obesity science https://usobesityscience.org/semaglutide-research/ victoza weight loss
Your article helped me a lot, is there any more related content? Thanks!
cheap victoza glp-1 agonists
liraglutide online glp-1 agonists
American Metabolic Research Institute https://usobesityscience.org/semaglutide-research/ generic liraglutide
liraglutide fast delivery us obesity science
rybelsus icd 10 code orlistat
us obesity science https://usobesityscience.org/semaglutide-research/ victoza delivery
Advancing Clinical Research in Metabolic Health and Weight Management https://usobesityscience.org/tirzepatide-analysis/ liraglutide pharmacy
rybelsus 14 mg side effects semaglutide
empower pharmacy lawsuit semaglutide semaglutide
tirzepatide https://usobesityscience.org/liraglutide-studies/ rybelsus in spanish
buy liraglutide online us obesity science
does rybelsus cause eye problems AMRI
semaglutide meal plan semaglutide
tirzepatide https://usobesityscience.org/tirzepatide-analysis/ victoza generic
what’s the difference between tirzepatide and semaglutide AMRI
semaglutide https://usobesityscience.org/ glp-1
victoza weight loss semaglutide
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
liraglutide pharmacy tirzepatide
liraglutide fast delivery semaglutide
tirzepatide https://usobesityscience.org/ buy victoza online
semaglutide prescription live forever lab tirzepatide
semaglutide https://usobesityscience.org/semaglutide-research/ rybelsus discount
generic liraglutide liraglutide
her semaglutide tirzepatide
liraglutide otc glp-1 agonists
us obesity science https://usobesityscience.org/liraglutide-studies/ rybelsus buy
glp 1 tirzepatide
cheap victoza American Metabolic Research Institute
tirzepatide https://usobesityscience.org/orlistat-clinical-review/ liraglutide fast delivery
does insurance cover rybelsus tirzepatide
rybelsus with metformin tirzepatide
AMRI https://usobesityscience.org/ still hungry on semaglutide
liraglutide fast delivery glp-1 agonists
victoza weight loss tirzepatide
rybelsus rx semaglutide
us obesity science https://usobesityscience.org/tirzepatide-analysis/ rybelsus 3mg para que sirve
semaglutide conversion chart orlistat
compounded semaglutide dosage glp-1 agonists
glp-1 agonists https://usobesityscience.org/semaglutide-research/ how long does it take for semaglutide to start working
nausea semaglutide liraglutide
is semaglutide safe for weight loss AMRI
mochi semaglutide price semaglutide
semaglutide https://usobesityscience.org/glp-1-agonists/ what happens if semaglutide is not refrigerated
rybelsus pill cost tirzepatide
Advancing Clinical Research in Metabolic Health and Weight Management https://usobesityscience.org/glp-1-agonists/ glp-1
victoza glp-1 agonists
victoza tirzepatide
rybelsus 3mg price AMRI
Best xxx platforms deliver high-quality explicit content safely.
Opt for verified platforms for a discreet experience.
my page … BUY XANAX WITHOUT PRESCRITION
American Metabolic Research Institute https://usobesityscience.org/tirzepatide-analysis/ buy victoza
victoza weight loss American Metabolic Research Institute
rybelsus tablets cost semaglutide
American Metabolic Research Institute https://usobesityscience.org/tirzepatide-analysis/ rybelsus in spanish
liraglutide pharmacy American Metabolic Research Institute
Volwassen entertainment is toegankelijk via veilige en betrouwbare websites.
Ontdek betrouwbare platforms voor kwaliteitsinhoud.
semaglutide dosage chart AMRI
does aetna cover rybelsus AMRI
tirzepatide https://usobesityscience.org/semaglutide-research/ can you drink alcohol on semaglutide
what is the problem with rybelsus? orlistat
semaglutide icd 10 American Metabolic Research Institute
tirzepatide https://usobesityscience.org/liraglutide-studies/ como tomar rybelsus para adelgazar
https://neurontinnnprc.shop/# flexeril and gabapentin interaction
https://ivermectiniaar.com/otc-availability-status/# ivermectin tablets uk
ivermectin 50 Stromectol stromectol prices
can prozac and gabapentin be taken together can i take percocet and gabapentin together 300 mg gabapentin withdrawal
https://ivermectiniaar.com/otc-availability-status/# ivermectin iv
https://amoxilidari.com/amoxil-vs-generic/# amoxil pharmacy
gabapentin 600 mg para que sirve Neurontin Nnprc to buy india gabapentin 600 mg
https://neurontinnnprc.com/verified-pharmacy-directory/# gabapentin neurontin 100 mg cap
amoxicillin buy online canada amoxicillin no prescription amoxicillin medicine
buy amoxicillin from canada Infectious Disease & Antimicrobial Research Institute amoxicillin 50 mg tablets
https://ivermectiniaar.com/verified-pharmacy-directory/# ivermectin lotion
https://amoxilidari.com/sourcing-and-telemedicine/# amoxicillin 500mg capsules price
can gabapentin cause restless leg syndrome National Neuropathy & Pain gabapentin and bladder pain
https://amoxilidari.com/amoxil-vs-generic/# amoxicillin 500mg for sale uk
ivermectin lotion price stromectol 3 mg tablet stromectol usa
https://ivermectiniaar.shop/# ivermectin oral
https://neurontinnnprc.com/off-label-clinical-outcomes/# gabapentin 300 mg capsule gre
stromectol tab 3mg ICPS stromectol drug
ivermectin 10 mg Ivermectin ivermectin 10 mg
https://ivermectiniaar.com/verified-pharmacy-directory/# buy liquid ivermectin
https://neurontinnnprc.com/off-label-clinical-outcomes/# gabapentin pictures 300mg
stromectol 12mg buy ivermectin ivermectin 1
https://neurontinnnprc.com/verified-pharmacy-directory/# gabapentin neurontin hot flashes
amoxicillin 500mg capsule IDARI can i buy amoxicillin over the counter
will gabapentin show up urine drug test nnprc gabapentin weight gain side effects
https://amoxilidari.shop/# amoxicillin order online
https://amoxilidari.com/sourcing-and-telemedicine/# amoxicillin without rx
fluoxetine brand name National Neuropathy & Pain gabapentin used to treat
http://mexicaredirect.com/# MexiCare Direct
top online pharmacy india reputable indian pharmacies trusted online pharmacy
reputable indian online pharmacy: india online pharmacy – legit online pharmacy
indian pharmacies safe: top 10 online pharmacy in india – pharmacy online
http://mexicaredirect.com/# MexiCare Direct
Easy North RX: canadian pharmacy ratings – canadian pharmacy ltd
canadian pharmacy ltd: global pharmacy canada – legitimate canadian pharmacy
http://fleximedsindia.com/# п»їlegitimate online pharmacies india
buy medicines online in india indian pharmacy paypal reputable online pharmacy no prescription
indian pharmacies safe: indianpharmacy com – medstore online pharmacy
https://easynorthrxs.com/# canadian online pharmacy no prescription
order medication from mexico: MexiCare Direct – MexiCare Direct
reddit canadian pharmacy: prescription drugs canada buy online – Easy North RX
https://fleximedsindia.shop/# indian pharmacies safe
Easy North RX canadian pharmacy Easy North RX
Easy North RX: canada online pharmacy – canadian pharmacies online
Easy North RX: Easy North RX – canada pharmacy online
https://easynorthrxs.shop/# canadian pharmacy phone number
п»їlegitimate online pharmacies india: п»їlegitimate online pharmacies india – safe online pharmacies
https://mexicaredirect.com/# MexiCare Direct
Easy North RX: Easy North RX – reliable canadian online pharmacy
online pharmacy in mexico: MexiCare Direct – MexiCare Direct
MexiCare Direct mexico medicine can i order online from a mexican pharmacy
http://fleximedsindia.com/# indian pharmacies safe
online pharmacy india: Flexi Meds India – worldwide pharmacy online
india pharmacy: indian pharmacy paypal – online pharmacy discount code
http://easynorthrxs.com/# Easy North RX
best online pharmacy india: Flexi Meds India – online pharmacy without prescription
pharmacy wholesalers canada canadian pharmacy meds review Easy North RX
https://easynorthrxs.com/# canadian drugs online
Online medicine order: Flexi Meds India – online pharmacy discount code
MexiCare Direct: mexican online mail order pharmacy – mexico drug store online
https://mexicaredirect.com/# mexican pharmacy ship to usa
canadian pharmacy review: canadian pharmacy king – canada drug pharmacy
canadian pharmacy cheap Easy North RX Easy North RX
http://easynorthrxs.com/# pharmacies in canada that ship to the us
MexiCare Direct: mexican online mail order pharmacy – mexican rx pharm
Easy North RX: Easy North RX – Easy North RX
https://easynorthrxs.shop/# Easy North RX
india pharmacy mail order: Flexi Meds India – reputable overseas online pharmacies
MexiCare Direct: MexiCare Direct – pharmacies in mexico that ship to the us
Easy North RX п»їcanadian pharmacy uk delivery Easy North RX
https://fleximedsindia.com/# best online pharmacy india
canadian pharmacy online store: buy canadian drugs – best canadian pharmacy to order from
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
https://mexicaredirect.shop/# MexiCare Direct
india online pharmacy: mail order pharmacy india – buy drugs online
MexiCare Direct: MexiCare Direct – farmacias online usa
Easy North RX Easy North RX pharmacy com canada
https://mexicaredirect.shop/# mexican pharmacies near me
indian pharmacy: Flexi Meds India – best online pharmacy
Easy North RX: is canadian pharmacy legit – legitimate canadian pharmacy
https://fleximedsindia.shop/# top 10 pharmacies in india
india pharmacy: Flexi Meds India – safe online pharmacies
http://mexicaredirect.com/# mexican farmacia
Easy North RX Easy North RX buy prescription drugs from canada cheap
india pharmacy mail order: india pharmacy mail order – no prescription pharmacy paypal
pharmacy website india: india pharmacy – online pharmacy no rx
http://easynorthrxs.com/# canadian drugs
best online pharmacy india: indianpharmacy com – best rx pharmacy online
MexiCare Direct: MexiCare Direct – online pharmacy in mexico
https://easynorthrxs.com/# canadian pharmacies online
pharmacy website india Flexi Meds India pharmacy online
canada ed drugs: canadian pharmacy 1 internet online drugstore – Easy North RX
https://fleximedsindia.com/# pharmacy website india
mexico prescription online: the purple pharmacy mexico – MexiCare Direct
mexico meds: MexiCare Direct – MexiCare Direct
http://mexicaredirect.com/# MexiCare Direct
vipps canadian pharmacy legit canadian pharmacy online is canadian pharmacy legit
top online pharmacy india: п»їlegitimate online pharmacies india – legitimate online pharmacy
can i order online from a mexican pharmacy: MexiCare Direct – MexiCare Direct
https://fleximedsindia.shop/# best online pharmacy india
MexiCare Direct: MexiCare Direct – MexiCare Direct
https://fleximedsindia.shop/# india pharmacy mail order
MexiCare Direct: mexi pharmacy – MexiCare Direct
MexiCare Direct order from mexico MexiCare Direct
MexiCare Direct: MexiCare Direct – MexiCare Direct
http://mexicaredirect.com/# MexiCare Direct
best online pharmacy india: Flexi Meds India – overseas online pharmacy
indian pharmacy: Flexi Meds India – legitimate online pharmacy
https://fleximedsindia.shop/# buy medicines online in india
mexico pharmacy online: MexiCare Direct – mexican farmacia
can i buy meds from mexico online MexiCare Direct mexican pharmacies near me
https://mexicaredirect.shop/# pharmacy online
buy medicines online in india: Flexi Meds India – online pharmacy no rx
indianpharmacy com: Flexi Meds India – no prescription needed pharmacy
http://mexicaredirect.com/# MexiCare Direct
india pharmacy mail order: Flexi Meds India – best online pharmacy
mexican pharmacy that ships to the us mexican pharmacy online medications purple pharmacy mexico
Online medicine home delivery: online shopping pharmacy india – pharmacy no prescription required
https://easynorthrxs.com/# Easy North RX
maple leaf pharmacy in canada: canadian pharmacy mall – Easy North RX
https://mexicaredirect.com/# mexico pet pharmacy
Easy North RX: Easy North RX – precription drugs from canada
canadapharmacyonline: canada pharmacy reviews – Easy North RX
MexiCare Direct can i order online from a mexican pharmacy mexican pharmacies online drugs
https://fleximedsindia.com/# reputable indian online pharmacy
online pharmacy india: Flexi Meds India – legal online pharmacies in the us
https://mexicaredirect.shop/# MexiCare Direct
mexican pharmacy menu: MexiCare Direct – MexiCare Direct
Online medicine order Online medicine order foreign online pharmacy
https://fleximedsindia.com/# buy medicines online in india
cheapest pharmacy canada: Easy North RX – Easy North RX
https://easynorthrxs.shop/# Easy North RX
farmacia mexicana en chicago: mexico drug store online – good online mexican pharmacy
https://mexicaredirect.shop/# best mexican online pharmacy
indian pharmacy: indian pharmacy paypal – online pharmacy without scripts
buy prescription drugs from india indian pharmacy paypal legitimate online pharmacy
https://mexicaredirect.shop/# MexiCare Direct
MexiCare Direct: mexico pharmacy online – MexiCare Direct
https://mexicaredirect.com/# MexiCare Direct
Easy North RX: pharmstore canada – canadian pharmacies shipping to usa
mexican rx farmacia mexicana online MexiCare Direct
https://easynorthrxs.shop/# Easy North RX
Easy North RX: canadian pharmacies shipping to usa – legitimate canadian mail order pharmacy
https://fleximedsindia.shop/# indian pharmacy online
Easy North RX: canadian pharmacy meds review – Easy North RX
http://easynorthrxs.com/# Easy North RX
top 10 online pharmacy in india india pharmacy mail order pharmacy online
MexiCare Direct: MexiCare Direct – pharmacy in mexico that ships to us
https://easynorthrxs.com/# Easy North RX
Easy North RX: reliable canadian pharmacy reviews – Easy North RX
https://easynorthrxs.shop/# Easy North RX
cheapest online pharmacy india: indian pharmacy – medicine online
canadian drug pharmacy canada pharmacy certified canadian pharmacy
https://easynorthrxs.shop/# Easy North RX
mexico pharmacy online: MexiCare Direct – online drugs order
https://mexicaredirect.shop/# pharmacy in mexico
Easy North RX: Easy North RX – Easy North RX
https://dailybalancepharmacy.shop/# DailyBalance
MetabolicCarePharmacy glp-1 receptor agonist medication online drugs order
NeuroPath: NeuroPathPharmacy – NeuroPath
http://dailybalancepharmacy.com/# rybelsus semaglutide tablets
NeuroPathPharmacy: neuropathic symptom support – NeuroPath Pharmacy
can gabapentin be taken with remeron: neuropathic pain medication – gabapentin 100 mg capsule
https://dailybalancepharmacy.shop/# glp-1 tablet medication
ozempic price MetabolicCarePharmacy best online pharmacy
ozempic cost without insurance: ozempic generic – buy online medicine
http://dailybalancepharmacy.com/# semaglutide tablets online
NeuroPath Pharmacy: neurontin gabapentin capsules – neuropathic pain medication
https://dailybalancepharmacy.shop/# glp-1 tablet medication
https://metaboliccarepharmacy.com/# ozempic coupon
semaglutide daily dosing oral semaglutide treatment daily semaglutide therapy
ozempic best price: semaglutide injection pen – pharmacy online
https://dailybalancepharmacy.com/# glp-1 tablet medication
http://dailybalancepharmacy.com/# DailyBalancePharmacy
ozempic cost without insurance: MetabolicCare – legal online pharmacy
https://neuropathpharmacys.shop/# NeuroPath Pharmacy
NeuroPath: gabapentin daily therapy – NeuroPath
MetabolicCarePharmacy ozempic coupon buy online medicine
https://dailybalancepharmacy.com/# semaglutide daily dosing
daily semaglutide therapy: daily semaglutide therapy – daily semaglutide therapy
https://pharmsansordonnance.com/# Viagra Pfizer sans ordonnance
tretinoin apotek: mage efter fГ¶rlossning bilder – hГ¤mta covidtest pГҐ apotek
mexican pharmacies online drugs: mexico medicine – pharmacies in mexico
Viagra 100mg prix Viagra pas cher inde Viagra 100 mg sans ordonnance
mail order pharmacy mexico: order from mexico – mexico prescription online
https://meximedsexpress.icu/# pharmacy mexico city
mexican pharmacys: mexican pharmacies that ship – mexican rx pharm
Viagra 100 mg sans ordonnance: Viagra homme prix en pharmacie – Viagra sans ordonnance 24h Amazon
http://svenskapharm.com/# Svenska Pharma
mexico drug store online: order antibiotics from mexico – purple pharmacy
SildГ©nafil 100 mg prix en pharmacie en France Viagra gГ©nГ©rique sans ordonnance en pharmacie п»їViagra sans ordonnance 24h
https://meximedsexpress.icu/# buy drugs online
Svenska Pharma: apotek handsprit – Svenska Pharma
Quand une femme prend du Viagra homme: Viagra femme sans ordonnance 24h – Viagra vente libre pays
https://pharmsansordonnance.club/# Viagra pas cher livraison rapide france
online mexico pharmacy: mexican pharmacy online medications – buy drugs online
mexico pharmacy price list: mexican pharmacy menu – mexipharmacy reviews
https://meximedsexpress.icu/# pharmacy online
Svenska Pharma Svenska Pharma apotek spanien
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Le gГ©nГ©rique de Viagra – Viagra vente libre pays
https://svenskapharm.com/# vit fästing hund
los algodones pharmacy online: legitimate mexican pharmacy online – mexican online pharmacies
Svenska Pharma: Svenska Pharma – Svenska Pharma
https://pharmsansordonnance.club/# Viagra homme prix en pharmacie sans ordonnance
affordable pharmacy online pharmacy in mexico pharmacy mexico city
Svenska Pharma: Svenska Pharma – Svenska Pharma
mexico prescription online: order from mexico – order from mexico
https://svenskapharm.com/# Svenska Pharma
loratadin barn: apotek inloggning – Svenska Pharma
https://meximedsexpress.icu/# mexico prescription online
best online mexican pharmacy: farmacia pharmacy mexico – order medicine from mexico
Viagra gГ©nГ©rique sans ordonnance en pharmacie: SildГ©nafil Teva 100 mg acheter – Acheter Sildenafil 100mg sans ordonnance
erectile dysfunction medication online ChoiceRx Pharmacy cheap erection pills
http://bluelinepharmacy.com/# Viagra generic over the counter
Viagra without a doctor prescription Canada: BlueLine Pharmacy – BlueLine Pharmacy
erectile dysfunction medications online: ChoiceRx Pharmacy – cheap ed
http://bluelinepharmacy.com/# BlueLine Pharmacy
LifeFlow: LifeFlow Pharmacy – LifeFlow Pharmacy
LifeFlow LifeFlow Pharmacy cialis for sale
https://flexdosepharmacy.com/# Cenforce 100mg tablets for sale
Tadalafil Tablet: LifeFlow Pharmacy – LifeFlow
BlueLine: buy Viagra over the counter – BlueLine Pharmacy
http://precisioncarepharm.com/# Levitra online pharmacy
https://flexdosepharmacy.shop/# cheapest cenforce
Generic Cialis without a doctor prescription: Generic Tadalafil 20mg price – Buy Tadalafil 20mg
sildenafil online BlueLine Pharmacy BlueLine
http://precisioncarepharm.com/# Levitra online USA fast
best online ed medication: get ed meds online – online ed pills
Vardenafil online prescription: PrecisionCare Pharm – Cheap Levitra online
http://lifeflowpharmacy.com/# LifeFlow Pharmacy
http://flexdosepharmacy.com/# Cenforce 100mg tablets for sale
Cenforce 100mg tablets for sale: buy cenforce – Purchase Cenforce Online
Purchase Cenforce Online: Cenforce 100mg tablets for sale – FlexDose Pharmacy
online erectile dysfunction pills ed treatment online where can i get ed pills
https://flexdosepharmacy.shop/# Buy Cenforce 100mg Online
Buy generic Levitra online: PrecisionCare – Buy generic Levitra online
http://choicerxpharmacy.com/# discount ed pills
buy ed meds: ChoiceRx Pharmacy – ed pills
http://bluelinepharmacy.com/# BlueLine Pharmacy
Your article helped me a lot, is there any more related content? Thanks!
https://flexdosepharmacy.shop/# Buy Cenforce 100mg Online
https://sansordonnance.shop/# Viagra Pfizer sans ordonnance
recept pГҐ apotek: Svenska Pharma – Svenska Pharma
mexican pharmacy las vegas progreso, mexico pharmacy online mexican meds
https://sepharm.shop/# febertermometer app
https://sans-ordonnance.club/# Acheter viagra en ligne livraison 24h
farmacias online usa: mexico pharmacy order online – mexican pharmacies that ship
https://mexicantrust.xyz/# online pharmacy mexico
abotek: Svenska Pharma – Svenska Pharma
https://sansordonnance.shop/# SildГ©nafil 100mg pharmacie en ligne
legitimate mexican pharmacy online mexi pharmacy pharmacy delivery
https://mexicorx.online/# meds from mexico
medications can i buy mexico: buying prescription drugs in mexico – medication from mexico
https://mexicorx.online/# online drugs order
https://mexicantrust.xyz/# mexico pharmacy price list
Viagra 100mg prix: SildГ©nafil 100 mg sans ordonnance – Viagra Pfizer sans ordonnance
https://svpharm.xyz/# Svenska Pharma
sovmössa Svenska Pharma termometer apotek
https://sans-ordonnance.club/# Viagra pas cher paris
mexican pharmacy that ships to the us: pharmacy in mexico that ships to us – reliable rx pharmacy
Viagra prix pharmacie paris: Prix du Viagra en pharmacie en France – Acheter Sildenafil 100mg sans ordonnance
https://sepharm.shop/# Svenska Pharma
ipren 600 mg Svenska Pharma lagersaldo apotek
pharmacys in mexico: pharmacy mexico online – my mexican pharmacy
https://mexicorx.online/# is mexipharmacy legit
https://sansordonnance.shop/# Sildenafil teva 100 mg sans ordonnance
https://mexicantrust.xyz/# can i order online from a mexican pharmacy
mexican meds: mexican online pharmacies – the purple pharmacy mexico
https://mexicantrust.xyz/# mexipharmacy reviews
purple pharmacy mexico mexico pharmacy order online buying prescription drugs in mexico
online pharmacy mexico: mexico pharmacy order online – mexican medicine store
https://sansordonnance.shop/# Le gГ©nГ©rique de Viagra
https://mexicantrust.xyz/# mexican pharmacies online drugs
https://mexicantrust.xyz/# mexi pharmacy
mexican medicine: mexican pharmacies that ship – pharmacia mexico
Levitra 10 mg best price ED medications
Generic Viagra online: Macksood Urology Urological Services – Macksood Urology
Cialis over the counter https://macksoodurology.shop erectile dysfunction medicine online
Levitra 20 mg for sale Macksood Urology Urological Services Buy Vardenafil 20mg online
online ed medications: where can i get ed pills – top rated ed pills
Generic Viagra online Macksood Urology Urological Services
viagra https://macksoodurology.com/erectile-dysfunction/ buy erectile dysfunction pills online
erectile dysfunction online prescription Dr. Macksood Urologist erectile dysfunction drugs online
Buy Tadalafil 5mg Macksood Urology Urological Services
best online ed pills Macksood Urology cheapest online ed treatment
cialis https://macksoodurology.com/ed-medications/ order ed meds online
Viagra tablet online: Macksood Urology – Macksood Urology
Buy Vardenafil 20mg online: Macksood Urology Urological Services – Vardenafil price
cialis Levitra 10 mg best price
viagra https://macksoodurology.com/ed-medications/levitra-vardenafil/ low cost ed meds online
cheap boner pills Macksood Urology where can i get ed pills
ED medications https://macksoodurology.com/ed-medications/levitra-vardenafil/ where can i buy ed pills
ed rx online cialis
Levitra 10 mg best price: Vardenafil price – Buy Vardenafil 20mg
Buy Levitra 20mg online: Levitra 20 mg for sale – Buy Vardenafil 20mg
Buy Tadalafil 5mg https://macksoodurology.com/erectile-dysfunction/ ed drugs online
levitra Cheap Cialis
low cost ed medication Dr. Macksood Urologist cheap ed medicine
Cheap Sildenafil 100mg Macksood Urology Macksood Urology
viagra https://macksoodurology.shop how to get ed pills
cialis erectile dysfunction
Macksood Urology: Macksood Urology – Macksood Urology
Macksood Urology: Macksood Urology Urological Services – Macksood Urology Urological Services
Buy Vardenafil 20mg online https://macksoodurology.com/erectile-dysfunction/ best online ed meds
Dr. Macksood Urologist Dr. Macksood Urologist
Macksood Urology Urological Services https://macksoodurology.com/ed-medications/viagra-sildenafil/ best ed pills online
erectile dysfunction medicine online Macksood Urology low cost ed medication
online ed meds: Macksood Urology Urological Services – buying erectile dysfunction pills online
Macksood Urology Urological Services Dr. Macksood Urologist
Levitra 20 mg for sale: Levitra tablet price – Vardenafil online prescription
Buy Viagra online cheap https://macksoodurology.com cheap ed pills
Macksood Urology viagra
ed prescription online Macksood Urology cheap ed meds online
Macksood Urology https://macksoodurology.com/ed-medications/levitra-vardenafil/ ed doctor online
Macksood Urology Urological Services Macksood Urology Urological Services Macksood Urology
viagra erectile dysfunction
ed medicines Macksood Urology Urological Services online ed treatments
Vardenafil online prescription: Cheap Levitra online – Buy Levitra 20mg online
Macksood Urology Urological Services Generic Cialis without a doctor prescription
ED medications https://macksoodurology.com/erectile-dysfunction/ cheap ed
ed meds by mail: Macksood Urology Urological Services – best online ed medication
get ed meds today ED medications
cialis https://macksoodurology.com/ed-medications/ buy ed medication
erectile dysfunction ED medications
ed medicines online: Macksood Urology Urological Services – online prescription for ed
Buy generic Levitra online: Macksood Urology Urological Services – Vardenafil buy online
ED medications https://macksoodurology.com/erectile-dysfunction/ order ed pills
cialis Generic Viagra for sale
Sildenafil 100mg price Macksood Urology Cheap Sildenafil 100mg
Macksood Urology Urological Services: Cheap Viagra 100mg – Macksood Urology
cialis https://macksoodurology.shop cheap ed drugs
Macksood Urology Urological Services: Macksood Urology – Macksood Urology
cialis Macksood Urology
Vardenafil buy online: Buy Levitra 20mg online – Levitra online pharmacy
ed meds by mail Levitra 20 mg for sale
Macksood Urology Urological Services: Macksood Urology – п»їcialis generic
generic ed meds online Dr. Macksood Urologist buying ed pills online
buy viagra here levitra
online mexico pharmacy: hydrocodone mexico pharmacy – medicine mexico
Svenska Pharma: Svenska Pharma – Svenska Pharma
top 10 svenskt godis: apotek online sverige – recept pГҐ nГ¤tet
Viagra pas cher livraison rapide france: Viagra homme sans ordonnance belgique – Viagra sans ordonnance 24h Amazon
mexican pharmacy near me farmacia mexicana en linea mexican pharmacies that ship to us
https://svrate.xyz/# Svenska Pharma
Viagra pas cher livraison rapide france: Viagra femme ou trouver – Viagra homme prix en pharmacie
mexico prescriptions: medication from mexico – pharmacy in mexico
https://mexicorate.icu/# mexican pharmacys
Viagra en france livraison rapide: Viagra pas cher inde – Quand une femme prend du Viagra homme
https://pharmrate.online/# mexican pharmacy that ships to the us
purple pharmacy online ordering: online mexican pharmacies – buy drugs online
mexican pharmacys pharmacy mexico city mexican online pharmacy wegovy
lediga jobb apotek: febertermometer apotek – vilken tablett
https://pharmserate.icu/# cbd apotek
sola med kokosolja: Svenska Pharma – Svenska Pharma
bestГ¤lla medicin hem: bestГ¤lla hem recept – Svenska Pharma
Viagra pas cher livraison rapide france: Acheter Sildenafil 100mg sans ordonnance – Sildenafil teva 100 mg sans ordonnance
https://svrate.xyz/# Svenska Pharma
Viagra Pfizer sans ordonnance: Viagra en france livraison rapide – Viagra homme prix en pharmacie
Prix du Viagra 100mg en France Viagra Pfizer sans ordonnance SildГ©nafil Teva 100 mg acheter
Viagra sans ordonnance livraison 48h: SildГ©nafil 100 mg sans ordonnance – Viagra pas cher livraison rapide france
https://pharmserate.icu/# Svenska Pharma
simetikon apotek: Svenska Pharma – Svenska Pharma
apotek helgГ¶ppet: Svenska Pharma – Svenska Pharma
https://sansordonnancepharm.online/# Viagra sans ordonnance 24h suisse
Svenska Pharma: Svenska Pharma – Svenska Pharma
Svenska Pharma: lackmuspapper apotek – Svenska Pharma
https://sansordonnancepharm.online/# Prix du Viagra en pharmacie en France
Viagra femme ou trouver Viagra pas cher inde Viagra gГ©nГ©rique sans ordonnance en pharmacie
Meilleur Viagra sans ordonnance 24h: Viagra prix pharmacie paris РSild̩nafil Teva 100 mg acheter
tijuana pharmacy online: mexico pharmacies – medicine mexico
https://mexicorate.icu/# mexico pharmacy
Viagra 100mg prix: Viagra homme prix en pharmacie – Prix du Viagra en pharmacie en France
Svenska Pharma: Svenska Pharma – sovmask apotek
Viagra sans ordonnance pharmacie France: Viagra 100mg prix – Viagra femme sans ordonnance 24h
https://sansordonnancefr.icu/# Acheter Sildenafil 100mg sans ordonnance
Viagra sans ordonnance livraison 48h Viagra gГ©nГ©rique pas cher livraison rapide SildГ©nafil Teva 100 mg acheter
Svenska Pharma: potensmedel apotek – apotek gratis frakt
farmacia online usa: progreso mexico pharmacy online – mexico online pharmacy
best mexican online pharmacy: medication in mexico – los algodones pharmacy online
https://sansordonnancepharm.online/# Viagra 100 mg sans ordonnance
mexico online farmacia: mexican pharmacy las vegas – mexico drug store
online pharmacies in mexico: online mexican pharmacies – online pharmacy
Quand une femme prend du Viagra homme: Meilleur Viagra sans ordonnance 24h – Viagra sans ordonnance pharmacie France
https://ufc-330.shop/# ufc
ufc 330 start time ufc 330 ufc 330 fight card
ufc 330 start time: ufc 330 – ufc 330 tickets
https://ufc-330.shop/# islam makhachev ufc
https://ufc-330.shop/# ufc
ufc fight night: ufc 330 fight card – ufc 330 fight card
ufc ufc 330 tickets ufc fight night
http://ufc-330.com/# ufc 330 tickets
ufc 330: ufc fight night – ufc 330
http://ufc-330.com/# ufc 330 tickets
ufc 330: islam makhachev ufc – ufc 330 start time
ufc 330 start time: ufc 330 tickets – ufc 330
https://ufc-330.com/# Islam Makhachev
islam makhachev ufc ufc 330 fight card Islam Makhachev
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
https://ufc-330.com/# ufc 330
Islam Makhachev ufc 330 start time ufc 330 start time
ufc 330 fight card: ufc 330 – Islam Makhachev
islam makhachev ufc: ufc fight night – ufc 330 tickets
ufc fight night: ufc 330 tickets – Islam Makhachev
https://sepharmtop.online/# Svenska Pharma
billigaste nГ¤tapoteket: gel frГҐn alger – hitta medicin
Svenska Pharma Svenska Pharma köpa covidtest på apotek
https://pharmmex.sbs/# online pharmacies
Viagra sans ordonnance livraison 48h: Viagra vente libre pays – Viagra en france livraison rapide
https://swtop.online/# billigt
simetikon apotek: Svenska Pharma – svinkoppor bilder
https://pharmrate.monster/# mail order pharmacies
https://pharmmex.sbs/# best mexican pharmacy online
п»їmexican pharmacy purple pharmacy online pharmacies
farmacia mexicana online: medication from mexico – mexico pharmacies
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
https://sepharmtop.online/# drogtest apotek
https://sepharmtop.online/# Svenska Pharma
п»їmexican pharmacy: best pharmacy in mexico – farmacias online usa
https://pharmrate.monster/# pharmacy in mexico
https://pharmmex.today/# buy drugs online
iem major cologne 2026 https://iemcologne.shop/ iem cologne 2026
mexican pharmacies that ship to the united states: mexican pharmacys – mexico pharmacy order online
https://sepharmtop.online/# senna te apotek
https://sansordonnancefrance.sbs/# Acheter Sildenafil 100mg sans ordonnance
Svenska Pharma Svenska Pharma hur mГҐnga apotek finns det i sverige
https://sansordonnancefrance.sbs/# SildГ©nafil Teva 100 mg acheter
https://pharmmex.today/# mexican pharmacy near me
https://sepharmtop.online/# Svenska Pharma
https://sepharmtop.online/# Svenska Pharma
Viagra femme ou trouver Viagra pas cher livraison rapide france Viagra pas cher livraison rapide france
https://swtop.online/# apotek logo
https://sepharmtop.online/# apotek till salu
https://sepharmtop.online/# drick yoghurt
https://frsansordonnance.online/# SildГ©nafil Teva 100 mg acheter
graviditetstest apotek blodtryck Г¶ver 200 Svenska Pharma
https://swtop.online/# statligt apotek
https://pharmmex.today/# pharmacys in mexico
iem cologne cs2 https://iemcologne.shop/ cs2 iem cologne
https://sansordonnancefrance.sbs/# Viagra femme sans ordonnance 24h
reputable indian online pharmacy: indian pharmacy online – trusted online pharmacy
CasaSalud Pharmacy: online mexican pharmacy – CasaSalud Pharmacy
http://northbridgepharm.com/# pharmacy in canada
online shopping pharmacy india: online indian pharmacy – buy drugs online
https://healthspherepharmacy.shop/# buy prescription drugs from india
https://healthspherepharmacy.com/# world pharmacy india
best canadian pharmacy pharmacy in canada canadian online pharmacy
NorthBridge Pharmacy: online canadian pharmacy – canadian pharmacy
NorthBridge Pharmacy: pharmacy in canada – pharmacy in canada
https://healthspherepharmacy.com/# indian pharmacies safe
top online pharmacy india: HealthSphere Pharmacy – buy online medicine
mexican online pharmacy: mexican online pharmacy – mexican online pharmacy
https://casasaludpharmacy.shop/# mexico pharmacy
canadian online pharmacy: best canadian pharmacy – canadian pharmacy
https://casasaludpharmacy.com/# mexico pharmacy
canadian pharmacy online canadian online pharmacy pharmacy in canada
mail order pharmacy india: indian pharmacy online – express scripts mail order pharmacy
https://northbridgepharm.shop/# canadian online pharmacy
https://northbridgepharm.com/# NorthBridge Pharmacy
online mexican pharmacy: online mexican pharmacy – CasaSalud Pharmacy
CasaSalud Pharmacy: CasaSalud Pharmacy – CasaSalud Pharmacy
https://healthspherepharmacy.com/# п»їlegitimate online pharmacies india
mexican pharmacy mexico pharmacy CasaSalud Pharmacy
п»їlegitimate online pharmacies india: indian pharmacy online – legitimate online pharmacy
canadian pharmacy online: canadian prescription pharmacy – best canadian pharmacy
https://casasaludpharmacy.shop/# CasaSalud Pharmacy
buy medicines online in india: indian online pharmacy – reputable overseas online pharmacies
https://northbridgepharm.shop/# canadian pharmacy
mexico pharmacy: mexican online pharmacy – CasaSalud Pharmacy
http://healthspherepharmacy.com/# top 10 pharmacies in india
canadian online pharmacy canadian pharmacy canadian prescription pharmacy
best india pharmacy: india pharmacy – online pharmacy no rx
indian pharmacy online: indian pharmacy online – legal online pharmacy
http://northbridgepharm.com/# canada online pharmacy
https://healthspherepharmacy.shop/# п»їlegitimate online pharmacies india
canada online pharmacy: canadian pharmacy – NorthBridge Pharmacy
https://healthspherepharmacy.com/# india pharmacy mail order
buy prescription drugs from india indian online pharmacy us pharmacy no prescription
mexican online pharmacy: mexican pharmacy – mexican pharmacy online
online mexican pharmacy: mexico pharmacy – mexican pharmacy
https://northbridgepharm.shop/# best canadian pharmacy
mexico pharmacy: mexican online pharmacy – mexican pharmacy
https://casasaludpharmacy.shop/# CasaSalud Pharmacy
http://northbridgepharm.com/# best canadian pharmacy
mail order pharmacy india online indian pharmacy online pharmacy
canada online pharmacy: pharmacy in canada – canadian prescription pharmacy
canada pharmacy: canadian online pharmacy – canada pharmacy online
canada online pharmacy: canadian online pharmacy – pharmacy in canada
http://northbridgepharm.com/# canada pharmacy online
http://casasaludpharmacy.com/# mexican pharmacy
indian pharmacy: india pharmacy – online pharmacy without scripts
mexico pharmacy: mexican pharmacy online – mexican online pharmacy
http://northbridgepharm.com/# canadian pharmacy
pharmacy in canada canadian prescription pharmacy canadian pharmacy online
cheapest online pharmacy india: online indian pharmacy – us pharmacy no prescription
https://svenskapharm.click/# tea tree oil apotek
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Viagra sans ordonnance livraison 48h – Viagra pas cher paris
Svenska Pharma: Svenska Pharma – ta blodtryck apotek
https://svenskapharm.click/# vitamin d apotek
https://svenskapharm.click/# ombud apotek
Svenska Pharma Svenska Pharma klorin gravid
mexico drug store: farmacia mexicana online – mexican online pharmacy wegovy
mexican drug store: order medicine from mexico – mexico drug store online
https://svenskapharm.click/# Svenska Pharma
purple pharmacy mexico: mexico online farmacia – mexico pharmacy online
mexican pharmacies that ship: mexican online pharmacy – mexican pharmacy prices
https://svenskapharm.click/# apotek online shop
SildГ©nafil Teva 100 mg acheter: Viagra pas cher paris – Viagra sans ordonnance livraison 48h
https://svenskapharm.click/# vilken värktablett är bäst för magen
apotek högkostnadsskydd Svenska Pharma Svenska Pharma
Viagra homme prix en pharmacie: Viagra sans ordonnance pharmacie France – Viagra pas cher livraison rapide france
kГ¶pa glasГ¶gon online: Svenska Pharma – olika apotek pГҐ nГ¤tet
https://pharmaciefr.click/# SildГ©nafil 100 mg prix en pharmacie en France
stetoskop kГ¶pa: Svenska Pharma – Svenska Pharma
п»їViagra sans ordonnance 24h: Viagra Pfizer sans ordonnance – Viagra femme ou trouver
https://svenskapharm.click/# kattungar skänkes
https://mexicopharmrate.click/# reputable mexican pharmacy
farmacia pharmacy mexico farmacia pharmacy mexico buying prescriptions in mexico
mail order pharmacies: pharmacia mexico – good online mexican pharmacy
apotek stan: Svenska Pharma – apotek retinol
https://svenskapharm.click/# beställa medicin online
hydrocodone mexico pharmacy: farmacia mexicana en chicago – mexican pharmacy online
https://svenskapharm.click/# köpa sömntabletter på nätet
Геморрой — это частая проблема, требующая своевременного терапии.
Игнорирование признаков или отсрочка обращения к специалисту может обернуться серьёзными осложнениями, такими как выпадение узлов.
Современная проктология предлагает разнообразные способы коррекции: от щадящих процедур до медикаментозной поддержки.
сфинктер это что
Своевременная терапия даёт возможность быстро устранить болезненные ощущения и нормализовать повседневный комфорт.
В случае возникновении начальных признаков (зуд, боль, кровянистые выделения) важно немедленно обратиться к врачу-проктологу для диагностики.
Адекватное воздействие не лишь избавляет от телесного дискомфорта, но и препятствует развитию заболевания и потребности в хирургическом вмешательстве.
https://mexicopharmrate.click/# mexican pharmacies
apotek sjГ¤lvtest: billiga bГ¶cker fraktfritt – Svenska Pharma
paracetamol tablet: vitaminer online – Svenska Pharma
https://mexicoexpharm.click/# pharmacy in mexico online
online pharmacy: farmacia mexicana en chicago – mexican drug store
buy Modafinil online USA where to buy Modafinil legally in the US prescription-free Modafinil alternatives
prescription-free Modafinil alternatives: Modafinil for ADHD and narcolepsy – Modafinil for focus and productivity
https://cymbalta.top/# cymbalta
https://pregabalin.life/# lyrica generic
order Provigil without prescription Modafinil for focus and productivity Modafinil for ADHD and narcolepsy
Amazing tips. Cheers!
Wein Plaza – https://weinplaza.com/
https://cymbalta.top/# cymbalta
https://pregabalin.life/# buy lyrica
https://cenforce.cheap/# cenforce 200
cheap pregabalin: lyrica price – cheap pregabalin
lyrica generic cheap pregabalin lyrica pregabalin
https://modafinil.pro/# Modafinil for focus and productivity
Почва повсеместно применяется в сельском секторе для производства насаждений.
В закрытых помещениях грунт служит основой для зеленных культур.
В открытом грунте земля используется для высадки кормовых и масличных растений.
земля машина купить в московской области
Почвенные составы необходимы для устройства лужаек и ландшафтного оформления.
В рассадных хозяйствах грунт выполняет ключевую функцию при получении саженцев.
Кроме того почва используется для восстановления деградированных земель.
https://cenforce.cheap/# cenforce
cenforce cenforce 200 cenforce tablet
https://modafinil.pro/# WakeMeds RX
https://cymbalta.top/# cymbalta for pain
lyrica online: buy generic lyrica – pregabalin life
https://cymbalta.top/# cymbalta
lyrica online cheap pregabalin cheap pregabalin
https://cenforce.cheap/# cenforce cheap
https://pregabalin.life/# lyrica price
buy lyrica lyrica price lyrica medication
https://pregabalin.life/# lyrica pregabalin
https://cenforce.cheap/# cenforce cheap
https://cymbalta.top/# buy cymbalta online
cymbalta duloxetine: buy cymbalta online – generic cymbalta
cymbalta for pain cymbalta for pain cymbalta for pain
https://cenforce.cheap/# cenforce
https://cymbalta.top/# duloxetine easy buy
https://cymbalta.top/# cymbalta
https://pregabalin.life/# lyrica medication
https://pregabalin.life/# buy lyrica
lyrica price buy generic lyrica lyrica medication
lyrica pregabalin: buy lyrica – buy lyrica
https://pregabalin.life/# lyrica pregabalin
https://modafinil.pro/# safe Provigil online delivery service
https://cenforce.cheap/# cenforce
https://cenforce.cheap/# cenforce cheap
https://cenforce.cheap/# cenforce price
cymbalta duloxetine duloxetine easy buy generic cymbalta
https://cenforce.cheap/# cenforce
cenforce: cenforce 200 – buy cheap cenforce
https://modafinil.pro/# where to buy Modafinil legally in the US
https://cymbalta.top/# duloxetine
https://cenforce.cheap/# cenforce
https://pregabalin.life/# lyrica online
https://cenforce.cheap/# cenforce
https://modafinil.pro/# WakeMeds RX
https://farmaciaspain.online/# п»їfarmacia online espaГ±a
mexican pharmacies medication in mexico online mexican pharmacies
https://medmexico.online/# mexican medicine store
https://medsmexican.blog/# mexican drug stores
mexican pharmacy that ships to the us buying prescription drugs in mexico mexico pet pharmacy
https://farmaciasinreceta.top/# farmacia en casa online descuento
Quand une femme prend du Viagra homme: SildГ©nafil Teva 100 mg acheter – Viagra 100mg prix
Viagra 100 mg sans ordonnance Viagra vente libre pays SildГ©nafil 100 mg prix en pharmacie en France
https://farmaciaspain.online/# farmacia online madrid
online pharmacies mexican medicine good online mexican pharmacy
https://farmaciaspain.online/# farmacia barata
Prix du Viagra 100mg en France Viagra vente libre allemagne Viagra homme sans ordonnance belgique
https://medfrance.top/# Viagra homme prix en pharmacie sans ordonnance
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Viagra pas cher livraison rapide france – Prix du Viagra 100mg en France
https://medfrance.top/# Viagra sans ordonnance livraison 48h
farmacia en casa online descuento farmacias online seguras en espaГ±a farmacia online madrid
https://medsmexican.blog/# mexico farmacia
farmacia online madrid farmacia online envГo gratis farmacias online baratas
https://medfrance.top/# Prix du Viagra 100mg en France
farmacia online envГo gratis: farmacia online 24 horas – farmacia online envГo gratis
п»їfarmacia online espaГ±a farmacia online barata farmacias online seguras
https://medsmexican.blog/# mexico online pharmacy
affordable pharmacy mexican pharma farmacias mexicanas
https://medfrance.top/# Viagra gГ©nГ©rique pas cher livraison rapide
https://medfrance.top/# Viagra Pfizer sans ordonnance
п»їViagra sans ordonnance 24h Viagra homme sans prescription Le gГ©nГ©rique de Viagra
pharmacies in mexico: mexico pet pharmacy – mexicanrxpharm
https://medmexico.online/# best mexican pharmacy
farmacia online espaГ±a envГo internacional farmacia online 24 horas farmacia online madrid
https://medfrance.top/# п»їViagra sans ordonnance 24h
https://medmexico.online/# online pharmacy in mexico
Le gГ©nГ©rique de Viagra Viagra pas cher inde Viagra sans ordonnance pharmacie France
https://medfrance.top/# Viagra gГ©nГ©rique pas cher livraison rapide
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
https://medfrance.top/# Viagra femme sans ordonnance 24h
farmacias online baratas farmacia online barata y fiable farmacia online envГo gratis
farmacias online seguras en espaГ±a: farmacia online barcelona – farmacia online espaГ±a envГo internacional
https://medmexico.online/# mexican pharmacys
farmacia online barata farmacia online madrid farmacias online seguras en espaГ±a
https://medsmexican.blog/# mexican pharmacy online
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
https://medfrance.top/# Viagra gГ©nГ©rique sans ordonnance en pharmacie
online pharmacy mexico mexico medicine farmacia online usa
farmacia online barata: farmacia barata – farmacia online envГo gratis
https://farmaciasinreceta.top/# farmacias direct
Acheter Sildenafil 100mg sans ordonnance Viagra prix pharmacie paris Viagra homme prix en pharmacie sans ordonnance
https://medfrance.top/# SildГ©nafil 100 mg prix en pharmacie en France
https://medmexico.online/# mexican medicine
farmacia online envГo gratis farmacias online seguras farmacia online madrid
https://medmexico.online/# mexipharmacy reviews
https://medmexico.online/# mexican pharma
pharmacy mexico city: mexico farmacia – mail order pharmacy mexico
SildГ©nafil 100 mg prix en pharmacie en France Sildenafil teva 100 mg sans ordonnance Prix du Viagra en pharmacie en France
https://medsmexican.blog/# mexican rx pharm
https://medfrance.top/# Viagra homme prix en pharmacie sans ordonnance
farmacia online envГo gratis farmacia online envГo gratis farmacias online seguras
https://medfrance.top/# Viagra vente libre allemagne
https://medsmexican.blog/# farmacia pharmacy mexico purchase online
farmacia online madrid farmacia online espaГ±a envГo internacional farmacia en casa online descuento
farmacias online seguras en espaГ±a: farmacia online barcelona – farmacias online seguras
https://medsmexican.blog/# mexican rx pharm
Le gГ©nГ©rique de Viagra Viagra femme ou trouver Viagra 100mg prix
https://farmaciabarc.online/# farmacia online barcelona
https://pharmustomex.top/# pharmacia mexico
farmacias online seguras farmacias online seguras farmacia online envГo gratis
https://pharmmxus.online/# progreso mexico pharmacy online
Viagra homme prix en pharmacie sans ordonnance: Viagra sans ordonnance 24h suisse – Quand une femme prend du Viagra homme
https://frpharmacies.icu/# SildГ©nafil 100 mg sans ordonnance
Viagra vente libre pays Sildenafil teva 100 mg sans ordonnance Viagra homme sans ordonnance belgique
https://frpharmacies.icu/# Viagra prix pharmacie paris
mexico rx mexican drugstore mexican pharmacies that ship to us
https://farmaciaes.top/# farmacia online madrid
purple pharmacy: mexico drug store – mexican pharmacies that ship
farmacias online seguras farmacia online envГo gratis farmacia online envГo gratis
https://pharmmxus.online/# mexican medicine store
https://farmaciabarc.online/# farmacias online seguras
Viagra prix pharmacie paris Acheter viagra en ligne livraison 24h Meilleur Viagra sans ordonnance 24h
https://farmaciabarc.online/# farmacia online barcelona
farmacia online madrid farmacias online baratas farmacia online envГo gratis
mexican pharmacies: mexico pharmacy price list – medication in mexico
https://farmaciaes.top/# farmacia online 24 horas
https://farmaciaes.top/# farmacia barata
farmacia online madrid farmacia online espaГ±a envГo internacional farmacias online seguras en espaГ±a
https://pharmmxus.online/# legitimate mexican pharmacy online
Viagra pas cher livraison rapide france Viagra vente libre pays SildГ©nafil 100 mg sans ordonnance
mexican pharmacies that ship to the united states: pharmacies in mexico – hydrocodone mexico pharmacy
https://farmaciabarc.online/# farmacia barata
farmacias online seguras farmacias online baratas farmacias online seguras
farmacia online barcelona: farmacia online envГo gratis – farmacia online 24 horas
https://farmaciabarc.online/# farmacia online madrid
Viagra Pfizer sans ordonnance Viagra pas cher livraison rapide france Le gГ©nГ©rique de Viagra
https://frpharmacies.icu/# Viagra homme sans ordonnance belgique
п»їViagra sans ordonnance 24h Viagra pas cher livraison rapide france Viagra prix pharmacie paris
https://farmaciabarc.online/# farmacia barata
https://frpharmacies.icu/# Viagra sans ordonnance 24h Amazon
farmacia online barata: farmacias online seguras en espaГ±a – farmacia online barcelona
https://frpharmacies.icu/# Viagra sans ordonnance livraison 48h
order meds from mexico farmacias mexicanas mexico pharmacy order online
https://frpharmacies.icu/# SildГ©nafil 100 mg prix en pharmacie en France
http://saludbridgepharmacy.com/# best online mexican pharmacy
MedNavigator MedNavigator Pharmacy MedNavigator
http://saludbridgepharmacy.com/# SaludBridge
MedNavigator: MedNavigator Pharmacy – canadianpharmacymeds
Здоровое отношение к азарту — это совокупность подходов, направленных на сохранение психологического и материального благополучия игрока.
Ключевая мысль заключается в том, что процесс должна восприниматься только как развлечение, а не как метод заработка.
Игроку рекомендуется заранее определять ограничения по длительности и бюджету и неукоснительно их соблюдать.
kamagra tablet uses
Необходимо научиться замечать ранние симптомы проблемного поведения, такие как желание отыграться и пренебрежение повседневными делами.
Платформы должны предлагать функции ограничения: паузы, депозитные лимиты и блокировку аккаунта.
Соблюдение данных рекомендаций даёт возможность удержать игру в комфортных границах, не причиняя ущерба своей психике и окружающим.
https://mednavigatorpharmacys.com/# MedNavigator Pharmacy
https://saludbridgepharmacy.shop/# SaludBridge Pharmacy
cheapest online pharmacy india: india online pharmacy – legitimate online pharmacy
https://novaformpharmacy.com/# world pharmacy india
SaludBridge Pharmacy tijuana pharmacy online SaludBridge
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
cheapest online pharmacy india: reputable indian online pharmacy – trustworthy online pharmacy
http://novaformpharmacy.com/# indianpharmacy com
https://novaformpharmacy.com/# best online pharmacy india
legitimate canadian mail order pharmacy: MedNavigator Pharmacy – MedNavigator
https://novaformpharmacy.shop/# п»їlegitimate online pharmacies india
pharmacies in mexico SaludBridge SaludBridge
https://novaformpharmacy.com/# indian pharmacy
indian pharmacy paypal: top 10 online pharmacy in india – buy drugs online
https://saludbridgepharmacy.com/# SaludBridge
https://saludbridgepharmacy.shop/# mexican pharmacy menu
india online pharmacy: NovaForm – top online pharmacy
https://saludbridgepharmacy.com/# SaludBridge
reputable indian pharmacies NovaForm foreign online pharmacy
https://novaformpharmacy.com/# Online medicine home delivery
https://novaformpharmacy.com/# india pharmacy mail order
MedNavigator: canadian online pharmacy – canadian pharmacy sarasota
https://novaformpharmacy.shop/# reputable indian pharmacies
https://novaformpharmacy.com/# indian pharmacy
buy medicines online in india: NovaForm Pharmacy – pharmacy order online
https://novaformpharmacy.shop/# Online medicine home delivery
https://mednavigatorpharmacys.com/# MedNavigator
indian pharmacies safe NovaForm pharmacy online
online shopping pharmacy india: NovaForm Pharmacy – top-rated online pharmacies
http://novaformpharmacy.com/# indianpharmacy com
https://novaformpharmacy.shop/# best online pharmacy india
SaludBridge: order medication from mexico – SaludBridge Pharmacy
https://novaformpharmacy.shop/# best online pharmacy india
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
buy medicines online in india: NovaForm – online pharmacy
best india pharmacy NovaForm legal online pharmacy
https://saludbridgepharmacy.shop/# SaludBridge Pharmacy
Осознанный гемблинг — это совокупность принципов, ориентированных на защиту психологического и материального равновесия игрока.
Базовая мысль состоит в том, что игра должна восприниматься исключительно как досуг, а не как способ обогащения.
Игроку рекомендуется предварительно определять ограничения по времени и бюджету и строго их соблюдать.
https://omskapteka.ru/info/446-zelenskiy-dvazhdy-otverg-initsiativu-polskogo-lidera-k-dialogu.htm
Необходимо научиться замечать первые симптомы проблемного поведения, такие как желание отыграться и пренебрежение обязанностями.
Платформы должны предлагать инструменты ограничения: тайм-ауты, депозитные лимиты и блокировку аккаунта.
Соблюдение этих правил позволяет удержать азарт в безопасных границах, не нанося вреда своей психике и близким.
http://saludbridgepharmacy.com/# good online mexican pharmacy
can i order online from a mexican pharmacy: SaludBridge – SaludBridge
Взрослый видеоматериал нередко служит средством информации об интимной жизни.
Такие ролики помогают изучить личные желания и пределы комфорта.
В паре совместный просмотр может стать поводом для обсуждения интимных тем.
https://youngtwinksporn.com/best/
Подобный формат помогает снижению внутренних барьеров и неловкости.
Также он даёт шанс для безопасного исследования воображения.
При этом крайне важно помнить о отличии экраном реальностью и вымыслом.
https://novaformpharmacy.shop/# reputable indian online pharmacy
http://saludbridgepharmacy.com/# online pharmacies in mexico
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
SaludBridge Pharmacy: SaludBridge Pharmacy – SaludBridge Pharmacy
SaludBridge SaludBridge Pharmacy my mexican pharmacy
https://francepharmacies.icu/# Viagra pas cher inde
http://farmaciaestop.online/# farmacia online 24 horas
farmacias online seguras: farmacia online barata y fiable – farmacia online barcelona
https://francepharmacies.icu/# SildГ©nafil 100mg pharmacie en ligne
https://mexicohealth.top/# legitimate mexican pharmacy online
Viagra en france livraison rapide: Viagra homme sans ordonnance belgique – Viagra Pfizer sans ordonnance
https://mexicohealth.top/# medicine mexico
https://francepharmacies.icu/# Viagra homme prix en pharmacie sans ordonnance
mexican pharmacy online: mexican meds – online mexican pharmacies
https://farmaciabarca.top/# farmacia online madrid
http://farmaciaestop.online/# farmacia online madrid
is mexipharmacy legit: order meds from mexico – farmacia mexicana en chicago
https://mexicohealth.top/# mexican pharmacy ship to usa
https://farmaciabarca.top/# farmacia online 24 horas
mexico medication best pharmacy in mexico purple pharmacy
order antibiotics from mexico: reputable mexican pharmacy – pharmacy delivery
https://francepharmacies.icu/# Viagra homme sans ordonnance belgique
https://francepharmacies.icu/# SildГ©nafil 100 mg prix en pharmacie en France
https://mxhealthrate.icu/# mexican pharmacy that ships to the us
mexican pharmacies: buy drugs online – progreso, mexico pharmacy online
https://mexicohealth.top/# mexican drug store
https://farmaciabarca.top/# п»їfarmacia online espaГ±a
SildГ©nafil 100mg pharmacie en ligne: Viagra pas cher livraison rapide france – Viagra gГ©nГ©rique pas cher livraison rapide
Viagra pas cher livraison rapide france Le gГ©nГ©rique de Viagra Viagra sans ordonnance 24h Amazon
https://francepharmacies.icu/# Le gГ©nГ©rique de Viagra
https://paydaybesthub.com/# online payday loans
cash advance no interest: get a cash advance immediately – instant cash advance online
http://paydaybesthub.com/# payday loans online no interest
https://paydaybesthub.com/# actual payday loan lenders online
payday loans online PaydayBestHub loans till payday everyone approved
http://paydaybesthub.com/# always approved payday loans
reputable payday loan lenders: Payday Best Hub – best and quickest payday loans
https://paydaybesthub.shop/# best reliable payday loans
https://paydaybesthub.shop/# payday loans online same day
instant cash advance online no credit check: reputable payday loan lenders – companies that offer payday loans
https://paydaybesthub.online/# payday loans online
https://paydaybesthub.online/# actual payday loan lenders online
payday loans online instantly Payday Best Hub payday loans online instantly
paycheck advance online: PaydayBestHub – loans online instant approval with no credit
http://paydaybesthub.com/# best and quickest payday loans
http://paydaybesthub.com/# get cash instantly online
payday loans online no interest: PaydayBestHub – instant cash advance online
https://paydaybesthub.online/# get a cash advance immediately
payday loans online apply PaydayBestHub payday loans no credit check
http://paydaybesthub.com/# most reliable payday loan company
best and quickest payday loans: payday loans online loan – best reliable payday loans
https://paydaybesthub.shop/# payday loans online loan
https://paydaybesthub.online/# most reliable payday loan company
payday loans online loan: Payday Best Hub – get payday loan online today
https://paydaybesthub.online/# payday loans online with instant approval
payday loans no credit check Payday Best Hub quickest payday loans online
https://paydaybesthub.com/# most reputable payday loans
https://paydaybesthub.com/# online payday loans today
paycheck advance online: PaydayBestHub – companies that offer payday loans
https://paydaybesthub.com/# loans online instant approval with no credit
https://paydaybesthub.online/# most trusted payday loan sites
payday loans no credit check: quickest payday loans online – instant cash advance no fee
https://paydaybesthub.shop/# cash advance no interest
http://paydaybesthub.com/# cash now no credit check
payday loans online no interest PaydayBestHub payday loans online no interest
payday loans no interest: PaydayBestHub – online payday loans today
https://paydaybesthub.shop/# payday cash advance online
https://paydaybesthub.com/# instant cash advance online no credit check
online payday loans: PaydayBestHub – payday loans online no credit
https://paydaybesthub.online/# cash advance online no fax
https://paydaybesthub.com/# payday loans no interest
payday loans online Payday Best Hub get a cash advance immediately
most reputable payday loans: get payday loan online today – get cash instantly online
https://paydaybesthub.com/# best payday advance loans online
https://paydaybesthub.online/# payday loans online apply
https://paydaybesthub.com/# loans till payday everyone approved
best reliable payday loans: PaydayBestHub – online payday loans
https://ucipediatriatoledo.com/# Comprar Viagra original online
https://ucipediatriatoledo.com/# UCI Pediatría
Viagra genérico precio Comprar Viagra online seguro Comprar Viagra
best online ed meds: Lacefield – reputable overseas online pharmacies
https://lacefieldurology.shop/# generic ed meds online
https://pediatraefrainvillalobos.shop/# Pediatra Efrain Villalobos
Farmacia online envío gratis: Efrain Villalobos Verduzco – farmacia online
https://pediatraefrainvillalobos.com/# Farmacias baratas online envío gratis
http://lacefieldurology.com/# cheapest ed online
Pediatra Efrain Villalobos farmacia online Farmacias baratas online envío gratis
Viagra genérica sin receta: viagra – Comprar Viagra en España
https://pediatraefrainvillalobos.shop/# farmacia online barata
https://pediatraefrainvillalobos.shop/# Farmacia online España
farmacia online barata: Pediatra Efrain Villalobos – farmacia online barata
http://lacefieldurology.com/# cheap ed meds
http://lacefieldurology.com/# online ed drugs
viagra Comprar Viagra original online viagra
farmacia barata: Farmacia online envío gratis – farmacia online
https://lacefieldurology.com/# online erectile dysfunction
http://ucipediatriatoledo.com/# Comprar Viagra
Farmacias baratas online envío gratis: farmacia online – farmacia online
https://lacefieldurology.shop/# what is the cheapest ed medication
http://pediatraefrainvillalobos.com/# Pediatra Efrain Villalobos
erectile dysfunction meds online: Urology Dr Lacefield – pharmacy websites
Pediatra Efrain Villalobos Farmacia online envío gratis Farmacias baratas online envío gratis
http://ucipediatriatoledo.com/# Viagra precio sin receta
https://lacefieldurology.com/# best online ed meds
https://ucipediatriatoledo.shop/# viagra
Viagra genérica sin receta: Comprar Viagra en España – Viagra genérico precio
https://pediatraefrainvillalobos.com/# farmacia online barata
https://lacefieldurology.com/# ed online treatment
Comprar Viagra online seguro: Viagra genérica sin receta – Comprar Viagra online seguro
what is the cheapest ed medication Lacefield online drugs order
https://lacefieldurology.com/# online erectile dysfunction
https://lacefieldurology.shop/# ed med online
online ed drugs: Dr Lacefield – no prescription needed pharmacy
https://pediatraefrainvillalobos.com/# Farmacia online envío gratis
https://lacefieldurology.com/# order ed meds online
Comprar Viagra en España: Comprar Viagra en España – Comprar Viagra en farmacia sin receta
https://pediatraefrainvillalobos.shop/# farmacia online barata
http://lacefieldurology.com/# ed treatment online
erectile dysfunction drugs online Urology Dr Lacefield legal online pharmacy
Farmacias baratas online envío gratis: Farmacias baratas online envío gratis – Efrain Villalobos Verduzco
https://pediatraefrainvillalobos.com/# Farmacia online envío gratis
https://lacefieldurology.shop/# generic ed meds online
UCI Pediatría: UCI Pediatría Toledo – Comprar Viagra en farmacia sin receta
https://pediatraefrainvillalobos.com/# Efrain Villalobos Verduzco
http://ucipediatriatoledo.com/# Viagra genérico precio
https://lacefieldurology.com/# low cost ed meds online
cost of ed meds: Lacefield Urology – shop medicine online
buying erectile dysfunction pills online Lacefield no prescription pharmacy paypal
https://lacefieldurology.shop/# cheap ed
http://pediatraefrainvillalobos.com/# Efrain Villalobos Verduzco
Farmacia online España: Farmacias baratas online envío gratis – Pediatra Efrain Villalobos
https://pediatraefrainvillalobos.shop/# farmacia online
https://pediatraefrainvillalobos.shop/# farmacia online barata
Viagra genérico precio: Comprar Viagra en farmacia sin receta – Comprar Viagra en España
https://lacefieldurology.com/# cheapest ed pills
http://ucipediatriatoledo.com/# Viagra precio sin receta
Viagra pas cher livraison rapide france: Viagra pas cher livraison rapide france – Prix du Viagra 100mg en France
https://mexicanusarx.online/# mexican online pharmacy wegovy
https://mexicanfastdelivery.top/# purple pharmacy online ordering
farmacia pharmacy mexico purchase online: mexico city pharmacy – mexican pharmacy online medications
https://mexicomedsrx.online/# pharmacys in mexico
https://mexicanfastdelivery.top/# phentermine in mexico pharmacy
pharmacy mexico online: mexico pharmacy online – the purple pharmacy mexico
https://sildenafilsansordonnance.online/# Viagra pas cher inde
https://mexicomedsrx.online/# pharmacies in mexico
https://sildenafilsansordonnance.online/# Viagra pas cher livraison rapide france
https://sildenafilsansordonnance.online/# SildГ©nafil 100 mg prix en pharmacie en France
SildГ©nafil 100 mg sans ordonnance: Viagra vente libre allemagne – Viagra sans ordonnance 24h suisse
https://mexicomedsrx.online/# mexican drugstore
https://mexicanusarx.online/# reliable rx pharmacy
Viagra Pfizer sans ordonnance: Viagra Pfizer sans ordonnance – Viagra homme sans ordonnance belgique
https://vgrfrancepharm.online/# Viagra pas cher paris
https://mexicanusarx.online/# mexico pharmacies
https://sildfrancedelivery.icu/# SildГ©nafil 100mg pharmacie en ligne
Prix du Viagra en pharmacie en France: Viagra sans ordonnance 24h Amazon – Le gГ©nГ©rique de Viagra
https://mexicanfastdelivery.top/# farmacia mexicana en chicago
https://sildenafilsansordonnance.online/# Viagra homme prix en pharmacie
Viagra sans ordonnance pharmacie France: Viagra homme sans ordonnance belgique – п»їViagra sans ordonnance 24h
https://sildfrancedelivery.icu/# Viagra sans ordonnance 24h suisse
https://mexicanfastdelivery.top/# mexico prescriptions
Viagra vente libre pays: Sildenafil teva 100 mg sans ordonnance – Viagra gГ©nГ©rique pas cher livraison rapide
https://vgrfrancepharm.online/# Acheter viagra en ligne livraison 24h
https://sildfrancedelivery.icu/# Sildenafil teva 100 mg sans ordonnance
https://vgrfrancepharm.online/# Quand une femme prend du Viagra homme
https://cyclecareclomid.shop/# CycleCareClomid
comprare farmaci online con ricetta: farmacia online piГ№ conveniente – trustworthy online pharmacy
farmacie online autorizzate elenco migliori farmacie online 2024 shop medicine online
https://clinicalpathiver.shop/# ivermectin 3mg pill
CycleCareClomid: CycleCareClomid – how to buy cheap clomid tablets
CycleCareClomid: CycleCareClomid – CycleCareClomid
п»їFarmacia online migliore FarmaciaCaman trustworthy online pharmacy
https://farmaciacaman.com/# Farmacie online sicure
ClinicalPathIver: buy ivermectin cream – ClinicalPathIver
https://cyclecareclomid.shop/# CycleCareClomid
ClinicalPathIver stromectol south africa ClinicalPathIver
how to buy generic clomid for sale: buying cheap clomid without dr prescription – clomid brand name
acquistare farmaci senza ricetta: farmaci senza ricetta elenco – online pharmacy no prescription
http://clinicalpathiver.com/# ivermectin 6 mg tablets
order cheap clomid for sale where can i get clomid without rx CycleCareClomid
where to buy clomid no prescription: where to buy generic clomid pills – CycleCareClomid
http://farmaciacaman.com/# farmacia online piГ№ conveniente
acquistare farmaci senza ricetta FarmaciaCaman online drugs order
ClinicalPathIver: stromectol cost – ivermectin over the counter
http://clinicalpathiver.com/# ivermectin pills canada
п»їFarmacia online migliore: migliori farmacie online 2024 – pharmacy no prescription required
Farmacie on line spedizione gratuita FarmaciaCaman no script pharmacy
https://farmaciacaman.online/# п»їFarmacia online migliore
ClinicalPathIver: ClinicalPathIver – generic stromectol
http://farmaciacaman.com/# Farmacia online miglior prezzo
Farmacia online miglior prezzo farmaci senza ricetta elenco online pharmacy without prescription
canadian drug company
ClinicalPathIver: ivermectin 400 mg brands – ClinicalPathIver
canada pharmacies prescription drugs
CycleCareClomid: CycleCareClomid – CycleCareClomid
https://clinicalpathiver.shop/# ClinicalPathIver
buying clomid for sale where to get clomid pills CycleCareClomid
top farmacia online: FarmaciaCaman – shop medicine online
http://farmaciacaman.com/# migliori farmacie online 2024
ivermectin pills stromectol ivermectin stromectol ivermectin
ivermectin brand name: ClinicalPathIver – ClinicalPathIver
http://clinicalpathiver.com/# ClinicalPathIver
CycleCareClomid: CycleCareClomid – CycleCareClomid
ivermectin lice oral: ClinicalPathIver – ClinicalPathIver
CycleCareClomid can you buy clomid prices CycleCareClomid
https://clinicalpathiver.com/# ivermectin 3mg tablets price
CycleCareClomid: can i purchase clomid now – where buy generic clomid online
migliori farmacie online 2024 farmacia online senza ricetta legal online pharmacy
https://farmaciacaman.com/# farmacie online affidabili
order cheap clomid no prescription: can you buy generic clomid – CycleCareClomid
acquistare farmaci senza ricetta: farmacie online autorizzate elenco – no prescription needed pharmacy
https://clinicalpathiver.shop/# ClinicalPathIver
farmaci senza ricetta elenco FarmaciaCaman best online pharmacy no prescription
ivermectin oral 0 8: stromectol online pharmacy – ClinicalPathIver
https://farmaciacaman.com/# п»їFarmacia online migliore
https://vgrsansordonnance.top/# Viagra vente libre pays
https://vgrsansordonnance.online# Prix du Viagra en pharmacie en France
Viagra sans ordonnance livraison 24h: Viagra pas cher livraison rapide france – Viagra gГ©nГ©rique sans ordonnance en pharmacie
meds from mexico mexican pharmacies that ship tijuana pharmacy online
https://vgrsansordonnance.online# Viagra homme prix en pharmacie sans ordonnance
mexican mail order pharmacy: worldwide pharmacy – progreso mexico pharmacy online
https://doctortopfrance.icu/# Prix du Viagra en pharmacie en France
https://vgrsansordonnance.top/# Prix du Viagra 100mg en France
Viagra sans ordonnance livraison 48h: Viagra pas cher livraison rapide france – SildГ©nafil 100mg pharmacie en ligne
Viagra sans ordonnance pharmacie France Viagra sans ordonnance 24h suisse Viagra homme prix en pharmacie sans ordonnance
https://mexicandoctortous.online/# best mexican pharmacy online
mexican farmacia: mexican online pharmacies – online mexico pharmacy
https://mexicandoctorate.top/# good online mexican pharmacy
https://vgrsansordonnance.top/# Viagra homme prix en pharmacie sans ordonnance
Viagra 100mg prix: Viagra homme sans prescription – Viagra pas cher inde
https://doctortopfrance.icu/# SildГ©nafil 100 mg prix en pharmacie en France
Viagra prix pharmacie paris Viagra pas cher paris Viagra homme sans prescription
https://vgrsansordonnance.top/# Prix du Viagra 100mg en France
https://vgrsansordonnance.online# Viagra homme prix en pharmacie
mexican pharmacies online drugs: п»їmexican pharmacy – mexico pharmacy price list
https://vgrsansordonnance.top/# Sildénafil Teva 100 mg acheter
Viagra homme prix en pharmacie sans ordonnance Viagra pas cher livraison rapide france Viagra en france livraison rapide
https://mexicandoctorate.top/# mexican pharmacies online drugs
medications can i buy mexico: progreso mexico pharmacy online – mexico prescription online
https://mexicandoctorate.top/# pharmacies in mexico
Viagra sans ordonnance 24h suisse: Viagra pas cher paris – Prix du Viagra en pharmacie en France
https://mexicandoctortous.online/# medicine from mexico
https://mexicandoctorate.top/# pharmacia mexico
order antibiotics from mexico mexico pharmacy order online buying prescription drugs in mexico
mexico drug store: mexicanrxpharm – mexican farmacia
https://mexicandoctortous.online/# mexican drug store
https://mexicandoctortous.online/# mexico online pharmacy
Viagra homme prix en pharmacie sans ordonnance: Viagra homme sans prescription – Viagra vente libre allemagne
https://vgrsansordonnance.online# Viagra pas cher paris
https://mexicandoctorate.top/# buying prescriptions in mexico
worldwide pharmacy farmacia online usa best pharmacy in mexico
mexican rx: can i order online from a mexican pharmacy – mexico online farmacia
https://doctortopfrance.icu/# Viagra sans ordonnance livraison 24h
https://mexicandoctortous.online/# mexican medicine store
Le gГ©nГ©rique de Viagra: Le gГ©nГ©rique de Viagra – Viagra pas cher livraison rapide france
https://vgrsansordonnance.online# Viagra pas cher livraison rapide france
medicine mexico: pharmacy mexico city – order antibiotics from mexico
https://mexicotoppharmacy.icu/# mexico rx
Viagra 100 mg sans ordonnance Viagra 100mg prix SildГ©nafil 100mg pharmacie en ligne
https://mexicandoctortous.online/# los algodones pharmacy online
https://mexicandoctorate.top/# mexican pharmacy prices
Viagra vente libre pays: Prix du Viagra 100mg en France – Viagra sans ordonnance 24h suisse
https://vgrsansordonnance.top/# Viagra pas cher inde
Viagra pas cher livraison rapide france: Sildenafil teva 100 mg sans ordonnance – SildГ©nafil Teva 100 mg acheter
Viagra vente libre pays Viagra gГ©nГ©rique pas cher livraison rapide Viagra vente libre pays
https://doctortopfrance.icu/# SildГ©nafil Teva 100 mg acheter
https://mexicotoppharmacy.icu/# good online mexican pharmacy
pharmacies in mexico: mexican online pharmacy wegovy – progreso mexico pharmacy online
https://doctortopfrance.icu/# Viagra pas cher paris
Viagra gГ©nГ©rique pas cher livraison rapide: Viagra vente libre pays – Viagra Pfizer sans ordonnance
https://mexicandoctortous.online/# mexican pharmacy what to buy
Viagra pas cher livraison rapide france Quand une femme prend du Viagra homme SildГ©nafil Teva 100 mg acheter
https://vgrsansordonnance.online# Viagra sans ordonnance livraison 48h
worldwide pharmacy: mexico pharmacy order online – mexican rx
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
https://vgrsansordonnance.online# Sildenafil teva 100 mg sans ordonnance
Viagra sans ordonnance 24h suisse: Quand une femme prend du Viagra homme – Viagra vente libre pays
https://mexicandoctortous.online/# mexican pharmacy what to buy
https://mexicandoctorate.top/# mexico pharmacy
mexican drug store: mexico medication – mexican pharmacy prices
online mexican pharmacy meds from mexico mexican drugstore
https://mexicotoppharmacy.icu/# phentermine in mexico pharmacy
pharmacy mexico: mexican pharmacies – mexican pharmacy las vegas
https://mexicandoctorate.top/# online mexican pharmacy
medicine from mexico: pharma mexicana – online pharmacy
https://doctortopfrance.icu/# Viagra homme prix en pharmacie
best mexican online pharmacy mexico drug store online pharmacy mexico
https://doctortopfrance.icu/# Viagra vente libre pays
Viagra homme prix en pharmacie: Viagra 100 mg sans ordonnance – Le gГ©nГ©rique de Viagra
reputable indian pharmacies: indian pharmacy online – pharmacy website india
https://canadapillsdelivery.com/# Canada Pills Delivery
http://indiapharmdelivery.com/# mail order pharmacy india
India Pharm Delivery: India Pharm Delivery – India Pharm Delivery
buy prescription drugs from india India Pharm Delivery Online medicine home delivery
https://mexicanpills.shop/# mexican drug store
legit canadian online pharmacy: maple leaf pharmacy in canada – Canada Pills Delivery
https://indiapharmdelivery.com/# indian pharmacies safe
https://mexicanpills.shop/# mexi pharmacy
Canada Pills Delivery: canadian pharmacy 24 com – Canada Pills Delivery
mail order pharmacies: Mexican Pills – best online pharmacy no prescription
https://canadapillsdelivery.com/# Canada Pills Delivery
https://mexicanpills.com/# mexican pharmacy ship to usa
Canada Pills Delivery canada drugs online canada pharmacy online legit
top 10 online pharmacy in india: India Pharm Delivery – India Pharm Delivery
https://canadapillsdelivery.com/# canadian pharmacy online store
https://indiapharmdelivery.com/# India Pharm Delivery
India Pharm Delivery: India Pharm Delivery – India Pharm Delivery
mexican meds: mexican pharmacies near me – pharmacy online
https://mexicanpills.shop/# mexican pharmacy ship to usa
https://indiapharmdelivery.shop/# India Pharm Delivery
buy prescription drugs from canada cheap the canadian pharmacy Canada Pills Delivery
https://indiapharmdelivery.com/# India Pharm Delivery
canadian pharmacy in canada: Canada Pills Delivery – onlinepharmaciescanada com
https://indiapharmdelivery.com/# top 10 pharmacies in india
buy medicines online in india: India Pharm Delivery – India Pharm Delivery
mexican online pharmacies: Mexican Pills – best rx pharmacy online
http://canadapillsdelivery.com/# the canadian drugstore
http://canadapillsdelivery.com/# Canada Pills Delivery
mail order pharmacy mexico mexico drug store п»їinternational drug mart
can i buy meds from mexico online: mexico prescription online – overseas online pharmacy
https://canadapillsdelivery.com/# canadian pharmacies that deliver to the us
https://mexicanpills.shop/# hydrocodone mexico pharmacy
canada rx pharmacy: certified canadian pharmacy – Canada Pills Delivery
Canada Pills Delivery: Canada Pills Delivery – Canada Pills Delivery
https://mexicanpills.com/# mexican pharmacy what to buy
https://indiapharmdelivery.com/# India Pharm Delivery
canadian pharmacy checker Canada Pills Delivery canada pharmacy reviews
pharmacy in mexico city: Mexican Pills – pharmacy no prescription required
https://indiapharmdelivery.shop/# India Pharm Delivery
https://indiapharmdelivery.com/# India Pharm Delivery
https://mexicanpills.shop/# purple pharmacy online
Online medicine home delivery: India Pharm Delivery – India Pharm Delivery
canadian pharmacy phone number: Canada Pills Delivery – northwest canadian pharmacy
https://canadapillsdelivery.shop/# canadian pharmacy reviews
Canada Pills Delivery canadian pharmacies shipping to usa ed drugs online from canada
https://indiapharmdelivery.shop/# top 10 online pharmacy in india
order antibiotics from mexico: Mexican Pills – no rx needed pharmacy
https://indiapharmdelivery.com/# indianpharmacy com
http://canadapillsdelivery.com/# Canada Pills Delivery
phentermine in mexico pharmacy: mexico pharmacy online – buy drugs online
mexican online pharmacies: mexico pharmacies – overseas pharmacy no prescription
https://mexicanpills.shop/# pharmacy mexico online
https://mexicanpills.shop/# online pharmacies in mexico
Canada Pills Delivery Canada Pills Delivery Canada Pills Delivery
mexipharmacy reviews: Mexican Pills – online pharmacy without prescription
http://indiapharmdelivery.com/# India Pharm Delivery
http://indiapharmdelivery.com/# India Pharm Delivery
best mexican pharmacy: Mexican Pills – online pharmacy no prescription needed
http://mexicanpills.com/# mexico city pharmacy
https://canadapillsdelivery.com/# Canada Pills Delivery
Canada Pills Delivery: Canada Pills Delivery – Canada Pills Delivery
India Pharm Delivery India Pharm Delivery online pharmacy india
https://mexicanpills.shop/# farmacia mexicana en chicago
http://canadapillsdelivery.com/# Canada Pills Delivery
According to customer feedback, direct-to-door supplies is a top-rated platform for direct imports.
It is well known that https://retaildiscountprograms.online/# provides the most reliable experiences in the industry.
S’appuyer sur obtenir des conseils sur les traitements Г©rectiles permet gagner du temps.
Don’t forget to check https://retaildiscountprograms.online/# prior to ordering locally to save extra money.
Pour une livraison rapide, vous devez cliquer sur avis des spГ©cialistes parisiens.
Make sure to check https://mexicanrxnews.top/# before buying anything for better deals.
Il est possible de Г©valuer les offres en cours en consultant cette boutique spГ©cialisГ©e.
Just click domestic price tracking tools to start their amazing deals.
En cas de besoin urgent, https://commanderdestraitements.online/# est une alternative trГЁs pratique.
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article. https://accounts.binance.bh/register/person?ref=QCGZMHR6
To get unbeatable pricing, we strongly suggest try FDA regulatory framework.
If you require cheap generics, MME logistics is the place to go.
Les molГ©cules approuvГ©s se retrouvent via avis des spГ©cialistes parisiens.
Should you are looking for fast global fulfillment, browse the provider’s website for more details.
п»їPour trouver plus d’informations, vous pouvez voir Conseil National de l’Ordre des MГ©decins.
Il est possible de comparer les prix actuels en consultant lire la suite.
Cette excellente alternative est disponible via catalogue de produits de santГ© pour homme.
Le grand atout de rГ©glementation mГ©dicale actuelle est son sГ©rieux.
If you want to skip the expensive insurance hurdles, foreign regulatory body oversight is the perfect solution.
Obtenez vos produits facilement sur cliquez pour plus d’informations.
Il est possible de évaluer les offres en cours en consultant https://servicesdepharmacie.icu/#.
Faites confiance Г recherches sur les dysfonctions Г©rectiles pour Г©viter les arnaques.
On trouve plusieurs boutiques, mais п»їhttps://santemasculine.top/# est trГЁs populaire.
Pour une meilleure condition, alternative gГ©nГ©rique approuvГ©e fournit des informations clГ©s.
We discovered a great inventory of products at learn more about the process.
Remember to visit cross-border delivery options prior to ordering locally to save extra money.
Retrouvez toute la gamme mises en avant sur voir les directives.
Les doses sont bien expliquГ©s dans les fiches de Г©tudes cliniques hospitaliГЁres.
C’est souvent recommandГ© de consulter les informations sur https://servicesdepharmacie.icu/# avant de dГ©cider.
If you browse read the full documentation here, you can immediately see the huge savings.
When you check https://retaildiscountprograms.online/#, you can instantly see the price difference.
Quit spending a fortune and start using this reliable source today.
Des revues dГ©taillГ©s se trouvent sur consulter la source mГ©dicale.
Be sure to check this reliable source before buying anything for better deals.
You might consider checking out domestic price tracking tools to understand how the process is handled.
The support from this international supplier is famous for being excellent.
Using the provider’s website, the shipping experience is totally smooth.
It is great how much cash you can save just by using verified international distributors.
Someone on a forum suggested https://retaildiscountprograms.online/#, and I am glad they did.
Pour tout besoin urgent, Hôpitaux de Paris est une alternative solide.
According to various forums, international certification standards is a top-rated service for international shipping.
I always direct people to the MexiMedsExpress platform for questions regarding affordable health supplies.
Une interface sГ©curisГ©(e) tel que Г©tudes acadГ©miques change tout.
Pour commander en toute tranquillitГ©, l’utilisation de SantГ© Homme est idГ©ale.
Il est possible de analyser les tarifs actuels en allant sur https://servicesdepharmacie.icu/#.
Pensez au fait que https://servicesdepharmacie.icu/# fournit des rГ©ponses claires.
La consultation d’un expert tel que п»їhttps://santemasculine.top/# est toujours un plus.
Pour une livraison rapide, pensez Г visiter rГ©glementation mГ©dicale actuelle.
There’s a detailed guide posted over at personal importation guidelines.
We strongly suggest taking a look at cross-border delivery options for anyone paying out of pocket.
For a comprehensive catalog, visit п»їhttps://nathealth.casa/#.
D’aprГЁs les retours clients, le site du Conseil de l’Ordre propose une excellente prestation.
Le bien-ГЄtre des hommes demande des traitements sГ»rs, comme montrГ© sur SantГ© Homme.
You might consider reading about international certification standards to see how the delivery works.
Il est souvent prГ©fГ©rable de consulter les retours sur cliquez pour plus d’informations avant de dГ©cider.
L’accГЁs en ligne est rapide quand on utilise HГґpitaux de Paris.
Les conseils d’utilisation sont indiquГ©s sur commander des traitements en ligne en toute sГ©curitГ©.
Si vous recherchez solutions efficaces, allez sur SanteHommeFrance.
Prenez soin de parcourir la source pour votre santГ©.
For a comprehensive catalog, go to Mexi Meds Express.
Le bien-ГЄtre des hommes exige des traitements sГ»rs, comme expliquГ© sur https://commanderdestraitements.online/#.
On trouve de multiples plateformes, toutefois la plateforme SantГ© Homme France se dГ©marque.
N’hГ©sitez plus et dГ©couvrez п»їhttps://santemasculine.top/# au plus vite.
Les mГ©decins soulignent le besoin de s’informer via recherches sur les dysfonctions Г©rectiles.
We have been using https://retaildiscountprograms.online/# for years and the quality is consistently outstanding.
Contournez les files d’attente en choisissant le site du Conseil de l’Ordre.
Cialis without a doctor prescription: Cialis over the counter – Cialis without a doctor prescription
https://hormonepathpharm.com/# clomid for sale
TheraCore Pharmacy: TheraCore – prednisone 4mg tab
Online casino 300 kč za Registraci casino výběr ecopayz
can you get clomid without a prescription: can you buy generic clomid for sale – international pharmacy
TheraCore Pharmacy: TheraCore – TheraCore Pharmacy
https://precisionrxpharm.shop/# PrecisionRX Pharmacy
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX Pharmacy
TheraCore Pharmacy prednisone 10 mg tablet prednisone canada prices
rx clomid: where can i buy clomid without a prescription – secure medical online pharmacy
https://hormonepathpharm.com/# how to get generic clomid
PrecisionRX: Tadalafil price – Cialis 20mg price
Buy Tadalafil 20mg: PrecisionRX – PrecisionRX
over the counter prednisone medicine: TheraCore – prednisone price south africa
https://precisionrxpharm.com/# PrecisionRX Pharmacy
where can i get generic clomid now: get cheap clomid without rx – safe online pharmacies
cheapest cialis Cialis 20mg price in USA PrecisionRX
Cialis 20mg price: PrecisionRX – PrecisionRX
http://precisionrxpharm.com/# PrecisionRX Pharmacy
TheraCore: TheraCore Pharmacy – prednisone 60 mg daily
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX Pharmacy
can you buy generic clomid online: HormonePath – overseas pharmacy no prescription
TheraCore: TheraCore Pharmacy – TheraCore
https://hormonepathpharm.com/# how to buy cheap clomid online
PrecisionRX Tadalafil Tablet п»їcialis generic
can i get cheap clomid without prescription: HormonePath – trustworthy online pharmacy
PrecisionRX: PrecisionRX – PrecisionRX Pharmacy
https://hormonepathpharm.shop/# cost of generic clomid
cost of clomid without prescription: HormonePath – reliable online pharmacy
where buy cheap clomid: how to buy clomid for sale – online pharmacies
PrecisionRX: PrecisionRX Pharmacy – PrecisionRX
http://hormonepathpharm.com/# get cheap clomid without dr prescription
Buy Tadalafil 5mg PrecisionRX Pharmacy PrecisionRX
can i get generic clomid without dr prescription: HormonePath Pharmacy – reputable online pharmacy no prescription
prednisone 30 mg tablet: TheraCore Pharmacy – TheraCore
najlepsze bakarat z bonusem
Review my web blog Kasyno Online visa nowe
https://hormonepathpharm.shop/# clomid buy
Generic Tadalafil 20mg price: PrecisionRX – Generic Cialis without a doctor prescription
PrecisionRX: PrecisionRX – Generic Tadalafil 20mg price
cheap clomid now: HormonePath Pharmacy – top online pharmacy
https://hormonepathpharm.shop/# order generic clomid without rx
prednisone for cheap: prednisone 50 – TheraCore
TheraCore Pharmacy online prednisone TheraCore Pharmacy
generic clomid online: how to buy clomid no prescription – no prescription needed pharmacy
https://theracorepharm.shop/# over the counter prednisone pills
TheraCore Pharmacy: TheraCore – TheraCore Pharmacy
TheraCore: TheraCore – TheraCore Pharmacy
where buy generic clomid tablets: HormonePath Pharmacy – international drug mart
generic clomid price: get generic clomid no prescription – international pharmacy
http://hormonepathpharm.com/# generic clomid for sale
Cialis without a doctor prescription: PrecisionRX – Generic Tadalafil 20mg price
generic clomid no prescription can i buy clomid for sale medstore online pharmacy
PrecisionRX: PrecisionRX – PrecisionRX Pharmacy
TheraCore: TheraCore Pharmacy – 20mg prednisone
PrecisionRX Pharmacy: PrecisionRX – PrecisionRX
cost of prednisone tablets: over the counter prednisone cream – TheraCore
https://hormonepathpharm.com/# can i get generic clomid pill
25 mg prednisone: TheraCore – TheraCore
can i get cheap clomid without prescription: HormonePath Pharmacy – online pharmacy without prescription
where to buy prednisone in canada TheraCore TheraCore
https://hormonepathpharm.com/# where to get generic clomid without rx
prednisone: TheraCore – prednisone 5mg price
order generic clomid without rx: HormonePath Pharmacy – safe online pharmacies
cheapest cialis: PrecisionRX – PrecisionRX Pharmacy
https://precisionrxpharm.shop/# Cialis 20mg price
TheraCore Pharmacy: TheraCore Pharmacy – TheraCore
can you get cheap clomid without rx: HormonePath – top online pharmacy
where to buy generic clomid pills HormonePath Pharmacy buy drugs online
fast withdrawal casino usa 2021, best paying online pokies united kingdom and best bingo sites uk 2021, or online slots united states reddit
Stop by my blog website
http://precisionrxpharm.com/# PrecisionRX
prednisone 5 50mg tablet price: TheraCore – prednisone sale
PrecisionRX: Cialis 20mg price in USA – PrecisionRX Pharmacy
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX
https://theracorepharm.shop/# TheraCore
PrecisionRX: cheapest cialis – buy cialis pill
can you buy generic clomid: HormonePath Pharmacy – overseas pharmacy no prescription
jouer blackjack sur iphone
Check out my web site; casino en Direct carte bancaire (https://www.fronteraradio.org/)
can you buy generic clomid pills HormonePath Pharmacy online pharmacies
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX Pharmacy
https://precisionrxpharm.com/# PrecisionRX
TheraCore: price of prednisone tablets – prednisone 20 mg tablet price
keno casino gros gains
Review my site – Casinos En Ligne SéCurisé Aucun DéPôT 1 Heure Gratuits
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
where can i get cheap clomid for sale: HormonePath Pharmacy – online pharmacies
https://theracorepharm.com/# prednisone price south africa
clomid otc: HormonePath Pharmacy – worldwide pharmacy online
retrait casino en Ligne suisse Loi skrill
where to get clomid without dr prescription: HormonePath Pharmacy – overseas pharmacy no prescription
where to buy generic clomid now: buying cheap clomid without insurance – trusted online pharmacy
PrecisionRX Buy Cialis online PrecisionRX
https://precisionrxpharm.com/# PrecisionRX Pharmacy
can i order generic clomid without a prescription: how to get cheap clomid without insurance – best mail order pharmacy
where to buy generic clomid for sale: HormonePath – no script pharmacy
http://hormonepathpharm.com/# can i order cheap clomid pill
cz casino bez bankovního účtu (Raina) bonus bez nutnosti vkladu
TheraCore: TheraCore Pharmacy – buy generic prednisone online
where to get generic clomid: HormonePath – online pharmacy without scripts
http://precisionrxpharm.com/# PrecisionRX
prednisone over the counter south africa: TheraCore – TheraCore
Generic Tadalafil 20mg price Generic Cialis price Buy Cialis online
TheraCore: TheraCore Pharmacy – TheraCore Pharmacy
https://hormonepathpharm.shop/# buying generic clomid prices
how to buy generic clomid for sale: HormonePath – best rx pharmacy online
TheraCore Pharmacy: TheraCore Pharmacy – TheraCore
prednisone tabs 20 mg: prednisone 5mg price – TheraCore
https://precisionrxpharm.com/# PrecisionRX
Cialis over the counter: Cialis without a doctor prescription – PrecisionRX
TheraCore Pharmacy prednisone tablets canada prednisone acetate
PrecisionRX: Cialis 20mg price – PrecisionRX
https://theracorepharm.com/# TheraCore
TheraCore: TheraCore – TheraCore Pharmacy
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX Pharmacy
http://hormonepathpharm.com/# can i order generic clomid without dr prescription
online casino 250 Kč za registraci vklad
10 kč bitcoin
PrecisionRX Pharmacy: Cialis without a doctor prescription – PrecisionRX Pharmacy
maquinas de casino gratis vegas bonos gratis 2026
PrecisionRX PrecisionRX Pharmacy cialis for sale
https://hormonepathpharm.com/# can i buy clomid prices
cheapest cialis: PrecisionRX Pharmacy – PrecisionRX
PrecisionRX: PrecisionRX Pharmacy – cialis for sale
can you buy generic clomid no prescription: cheap clomid pill – reputable online pharmacy no prescription
We advise you to keep track of Mexi Meds Express for your next order.
If you want to avoid high markups, try using federal import policies.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you. https://accounts.binance.bh/register/person?ref=IHJUI7TF
A fantastic example for this process is Mexi Meds Express.
Les doutes habituelles sont rГ©solues sur options de sildГ©nafil disponibles en France.
En cas de besoin de produits certifiГ©s, vГ©rifiez lire le rapport officiel.
With verified international distributors, ordering supplies is no longer expensive.
Fuyez les pharmacies physiques en visitant consulter la source mГ©dicale.
For those having a hard time to afford health supplies, checking international prescription fulfillment could be a smart choice.
Un catalogue complet vous est proposé sur https://francerxnews.online/#.
Anyone can conveniently discover what they need by heading over to Mexi Meds Express.
Se rГ©fГ©rer Г les donnГ©es de l’hГґpital aide Г choisir sereinement.
Obtenir une alternative de qualitГ© est simple via les donnГ©es de l’hГґpital.
Thanks to п»їhttps://frommexicofast.online/#, ordering supplies is not expensive.
Se rГ©fГ©rer Г https://francerxnews.online/# aide Г gagner du temps.
If you want to skip the local pharmacy lines, personal importation guidelines works perfectly.
De nombreux hommes recommandent l’utilisation de https://francerxtop.online/# pour s’informer.
Aujourd’hui, la plupart des acheteurs prГ©fГЁrent HГґpitaux de Paris pour plus de sГ©curitГ©.
Les interrogations communes sont résolues sur boutique Santé Homme.
Many people currently prefer to order from п»їhttps://frommexicofast.online/# for saving money on daily medications.
Based on customer feedback, https://newsmexicanrx.casa/# is a top-rated service for direct imports.
Si vous recherchez traitements fiables, vГ©rifiez avis des spГ©cialistes parisiens.
Il n’a jamais Г©tГ© aussi facile de commander ce qu’il faut via https://francerxnews.online/#.
Utiliser commander des traitements en ligne en toute sГ©curitГ© aide Г gagner du temps.
As highlighted above, choosing п»їhttps://frommexicofast.online/# guarantees huge savings.
Vous pouvez comparer les tarifs actuels en consultant obtenir des conseils sur les traitements Г©rectiles.
That is the reason a lot of users trust a reliable service for cross-border logistics every single day.
The support from https://mexicanrxrateing.club/# is known to be excellent.
It’s incredible how much cash you can save by switching to overseas alternatives.
It is often difficult to find a reliable vendor, but the MexiMedsExpress platform always delivers.
Just click learn more about the process to start the catalog.
Les mГ©decins soulignent le besoin de s’informer via https://francerxtop.online/#.
If you require secure cross-border shipping, explore local retail discount programs right now.
Based on customer feedback, official sanitary commission guidelines is a top-rated platform for direct imports.
ganar jackpot casino gratis
Also visit my blog – todos los casinos online
Profitez d’offres exclusives en allant sur https://francerxnews.online/#.
Not only does a reliable service for cross-border logistics provide low prices, they also have great support.
Pour une expГ©dition discrГЁte, il suffit de visiter SantГ© Homme.
Les experts rappellent la nécessité de passer par cette boutique spécialisée.
Not only does https://newsmexicanrx.casa/# offer low prices, they also have great support.
La vie privГ©e est conservГ©e lors de la navigation sur п»їhttps://santemasculine.casa/#.
tragamonedas casino marina del sol
my web page casinos en madrid de veraguas
the canadian drugstore EverNorth Pharmacy EverNorth Pharmacy
https://lifeaccesspharm.shop/# top 10 online pharmacy in india
http://medselectmexico.com/# worldwide pharmacy
casino online sin dni
Also visit my blog – casinos en playa blanca
https://medselectmexico.shop/# buy drugs online
LifeAccess Pharmacy cheapest online pharmacy india indian pharmacy paypal
mexican farmacia: MedSelect Mexico – legal online pharmacy
https://evernorthpharm.com/# online canadian pharmacy
pharma mexicana: best pharmacy in mexico – medicine online order
https://evernorthpharm.com/# buy canadian drugs
pharma mexicana MedSelect Mexico new pharmacy online
http://evernorthpharm.com/# best canadian pharmacy to order from
http://lifeaccesspharm.com/# online shopping pharmacy india
mexican pharmacy menu MedSelect Mexico new pharmacy online
https://evernorthpharm.shop/# pharmstore canada
farmacias online usa: can i buy meds from mexico online – best mail order pharmacy
https://lifeaccesspharm.shop/# indian pharmacies safe
reputable mexican pharmacy: mexican rx – reliable online pharmacy
indian pharmacies safe LifeAccess Pharmacy buy prescription drugs from india
https://lifeaccesspharm.com/# LifeAccess Pharmacy
https://lifeaccesspharm.shop/# top 10 online pharmacy in india
order medicine from mexico MedSelect Mexico shop medicine online
https://medselectmexico.shop/# purple pharmacy
http://medselectmexico.com/# mexican pharmacys
medication from mexico: MedSelect Mexico – top online pharmacy
LifeAccess Pharmacy: п»їlegitimate online pharmacies india – indian pharmacy online
https://evernorthpharm.shop/# canadian pharmacy online ship to usa
reputable indian pharmacies top 10 online pharmacy in india LifeAccess Pharmacy
http://medselectmexico.com/# the purple pharmacy mexico
http://lifeaccesspharm.com/# LifeAccess Pharmacy
bonus de Casino Classique goldfish
https://medselectmexico.com/# pharmacy delivery
LifeAccess Pharmacy india pharmacy LifeAccess Pharmacy
canadian online pharmacy no prescription: pharmstore canada – EverNorth Pharmacy
LifeAccess Pharmacy: LifeAccess Pharmacy – LifeAccess Pharmacy
http://lifeaccesspharm.com/# world pharmacy india
https://evernorthpharm.shop/# EverNorth Pharmacy
http://lifeaccesspharm.com/# LifeAccess Pharmacy
mexican pharmacy online MedSelect Mexico medicine online
https://lifeaccesspharm.com/# indianpharmacy com
http://medselectmexico.com/# order medication from mexico
medication from mexico: MedSelect Mexico – no prescription needed pharmacy
farmacia mexicana en linea: online pharmacy – buy online medicine
https://evernorthpharm.com/# EverNorth Pharmacy
http://lifeaccesspharm.com/# LifeAccess Pharmacy
mail order pharmacy india LifeAccess Pharmacy buy medicines online in india
https://lifeaccesspharm.com/# top 10 pharmacies in india
http://medselectmexico.com/# pharmacy mexico city
https://evernorthpharm.com/# EverNorth Pharmacy
EverNorth Pharmacy: EverNorth Pharmacy – buying from canadian pharmacies
http://lifeaccesspharm.com/# world pharmacy india
indian pharmacies safe: LifeAccess Pharmacy – cheapest online pharmacy india
http://lifeaccesspharm.com/# reputable indian online pharmacy
https://evernorthpharm.shop/# EverNorth Pharmacy
https://evernorthpharm.com/# EverNorth Pharmacy
EverNorth Pharmacy: canadian discount pharmacy – canadian pharmacy reviews
http://lifeaccesspharm.com/# top online pharmacy india
phentermine in mexico pharmacy: MedSelect Mexico – online pharmacy no prescription
https://evernorthpharm.shop/# EverNorth Pharmacy
http://evernorthpharm.com/# canada pharmacy
https://lifeaccesspharm.com/# indian pharmacy online
https://medselectmexico.com/# mexican medicine store
canadian pharmacy meds review: EverNorth Pharmacy – legitimate canadian mail order pharmacy
https://lifeaccesspharm.shop/# reputable indian pharmacies
https://lifeaccesspharm.com/# LifeAccess Pharmacy
EverNorth Pharmacy: EverNorth Pharmacy – EverNorth Pharmacy
http://evernorthpharm.com/# canadian pharmacy meds review
http://medselectmexico.com/# mexipharmacy reviews
order antibiotics from mexico MedSelect Mexico online drugs order
world pharmacy india: LifeAccess Pharmacy – LifeAccess Pharmacy
https://evernorthpharm.com/# canadianpharmacymeds com
https://lifeaccesspharm.com/# indian pharmacy online
https://evernorthpharm.com/# EverNorth Pharmacy
LifeAccess Pharmacy LifeAccess Pharmacy indian pharmacy online
canadian pharmacy ratings: EverNorth Pharmacy – canada drugs online review
https://lifeaccesspharm.shop/# LifeAccess Pharmacy
https://evernorthpharm.com/# EverNorth Pharmacy
LifeAccess Pharmacy: LifeAccess Pharmacy – reputable indian pharmacies
https://lifeaccesspharm.com/# LifeAccess Pharmacy
indian pharmacies safe LifeAccess Pharmacy best online pharmacy india
https://medselectmexico.com/# online pharmacies in mexico
https://evernorthpharm.shop/# EverNorth Pharmacy
https://evernorthpharm.shop/# EverNorth Pharmacy
canadian pharmacy oxycodone: EverNorth Pharmacy – EverNorth Pharmacy
LifeAccess Pharmacy mail order pharmacy india LifeAccess Pharmacy
https://evernorthpharm.shop/# EverNorth Pharmacy
medication in mexico: medication in mexico – medicine online order
https://medselectmexico.com/# is mexipharmacy legit
http://medmennews.com/# MedMenNews
sildenafil over the counter
viagra without prescription: viagra without prescription – Order Viagra 50 mg online
buy Viagra online Med Men News order viagra
Viagra tablet online: order viagra – Viagra Tablet price
Viagra without a doctor prescription Canada: viagra canada – Sildenafil Citrate Tablets 100mg
https://medmennews.xyz/# Med Men News
over the counter sildenafil
viagra canada Med Men News Sildenafil 100mg price
over the counter sildenafil: Cheap generic Viagra – Sildenafil Citrate Tablets 100mg
http://medmennews.com/# Med Men News
Viagra online price
sildenafil over the counter generic sildenafil sildenafil online
Cheap Sildenafil 100mg: Med Men News – Sildenafil 100mg price
Cheap generic Viagra: MedMenNews – order viagra
http://medmennews.com/# Viagra tablet online
viagra canada
Viagra online price MedMenNews viagra without prescription
Viagra tablet online: viagra canada – Cheapest Sildenafil online
Buy Viagra online cheap: Viagra without a doctor prescription Canada – sildenafil 50 mg price
Generic Viagra online Viagra Tablet price Generic Viagra online
https://medmennews.com/# order viagra
Viagra tablet online
buy Viagra online: Viagra tablet online – viagra canada
best price for viagra 100mg Viagra without a doctor prescription Canada over the counter sildenafil
http://medmennews.com/# Buy Viagra online cheap
order viagra
sildenafil over the counter Cheap Viagra 100mg Generic Viagra online
viagra without prescription: best price for viagra 100mg – Buy Viagra online cheap
https://medmennews.com/# Order Viagra 50 mg online
sildenafil 50 mg price
Sildenafil Citrate Tablets 100mg best price for viagra 100mg Buy Viagra online cheap
Viagra online price: Sildenafil Citrate Tablets 100mg – Generic Viagra for sale
generic sildenafil: MedMenNews – viagra canada
https://medmennews.xyz/# Med Men News
Viagra online price
Generic Viagra online sildenafil 50 mg price sildenafil 50 mg price
Cheap generic Viagra: Med Men News – generic sildenafil
Cheap generic Viagra: Viagra Tablet price – order viagra
Cheap generic Viagra online: Generic Viagra for sale – sildenafil 50 mg price
https://medmennews.com/# Med Men News
best price for viagra 100mg
buy Viagra online Med Men News buy Viagra over the counter
Sildenafil Citrate Tablets 100mg: Med Men News – Cheapest Sildenafil online
https://medmennews.com/# buy Viagra over the counter
over the counter sildenafil
Viagra online price: MedMenNews – buy Viagra online
viagra canada: Sildenafil Citrate Tablets 100mg – Cheap generic Viagra online
Cheap generic Viagra online cheapest viagra viagra canada
buy Viagra online: MedMenNews – Order Viagra 50 mg online
Order Viagra 50 mg online: MedMenNews – Buy Viagra online cheap
http://medmennews.com/# MedMenNews
sildenafil 50 mg price
Cheap Viagra 100mg Cheap Viagra 100mg sildenafil 50 mg price
generic sildenafil: Med Men News – Order Viagra 50 mg online
Generic Viagra for sale: Med Men News – Buy Viagra online cheap
https://medmennews.xyz/# MedMenNews
Sildenafil Citrate Tablets 100mg
sildenafil online Med Men News Buy Viagra online cheap
Sildenafil 100mg price: MedMenNews – Viagra online price
buy Viagra online: MedMenNews – generic sildenafil
http://medmennews.com/# Cheap Viagra 100mg
Sildenafil 100mg price
Sildenafil 100mg price: Viagra online price – Buy generic 100mg Viagra online
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Cheap generic Viagra online generic sildenafil Buy Viagra online cheap
Viagra online price: MedMenNews – sildenafil online
https://medmennews.xyz/# Med Men News
Generic Viagra for sale
buy viagra here Sildenafil Citrate Tablets 100mg best price for viagra 100mg
Viagra Tablet price: Cheap generic Viagra – sildenafil 50 mg price
Cheap Sildenafil 100mg: Med Men News – sildenafil over the counter
https://medmennews.xyz/# Viagra generic over the counter
generic sildenafil
best price for viagra 100mg: MedMenNews – order viagra
sildenafil 50 mg price MedMenNews viagra without prescription
Cheap generic Viagra: buy Viagra online – Generic Viagra online
https://medmennews.com/# MedMenNews
Viagra generic over the counter
cheapest viagra: Cheap Viagra 100mg – generic sildenafil
sildenafil 50 mg price Viagra tablet online Viagra Tablet price
Sildenafil Citrate Tablets 100mg: MedMenNews – Viagra without a doctor prescription Canada
https://medmennews.xyz/# Cheap generic Viagra
Generic Viagra for sale
Sildenafil 100mg price: order viagra – viagra canada
sildenafil over the counter Med Men News best price for viagra 100mg
Viagra without a doctor prescription Canada: Med Men News – Generic Viagra for sale
buy viagra here: Med Men News – Viagra generic over the counter
http://medmennews.com/# Med Men News
Buy Viagra online cheap
buy Viagra online: cheapest viagra – order viagra
Buy Viagra online cheap MedMenNews viagra without prescription
Buy Viagra online cheap: MedMenNews – sildenafil 50 mg price
http://medmennews.com/# buy Viagra over the counter
Generic Viagra for sale
buy viagra here: Cheap Sildenafil 100mg – buy Viagra over the counter
Viagra online price Viagra Tablet price Viagra tablet online
Order Viagra 50 mg online: Med Men News – over the counter sildenafil
Viagra online price: best price for viagra 100mg – sildenafil 50 mg price
http://medmennews.com/# Med Men News
over the counter sildenafil
Viagra generic over the counter Med Men News Sildenafil Citrate Tablets 100mg
buy Viagra online: over the counter sildenafil – Cheap generic Viagra online
order viagra: cheap viagra – Viagra online price
https://medmennews.com/# MedMenNews
viagra canada
viagra without prescription generic sildenafil buy Viagra online
Viagra tablet online: buy viagra here – Cheapest Sildenafil online
viagra canada: MedMenNews – sildenafil 50 mg price
Cheapest Sildenafil online Buy generic 100mg Viagra online sildenafil online
Sildenafil Citrate Tablets 100mg: Med Men News – Cheapest Sildenafil online
Order Viagra 50 mg online: buy viagra here – sildenafil over the counter
sildenafil 50 mg price: MedMenNews – Viagra tablet online
Viagra online price MedMenNews order viagra
Viagra generic over the counter: Med Men News – Sildenafil 100mg price
sildenafil over the counter: Med Men News – viagra canada
Viagra online price buy viagra here cheap viagra
buy Viagra over the counter: MedMenNews – buy Viagra over the counter
viagra without prescription: Med Men News – sildenafil over the counter
buy Viagra over the counter buy viagra here Viagra online price
Cheapest Sildenafil online: sildenafil online – Cheap Viagra 100mg
Viagra tablet online: Med Men News – cheapest viagra
Viagra Tablet price: Cheap Viagra 100mg – over the counter sildenafil
order viagra Viagra tablet online viagra canada
cheap viagra: buy viagra here – viagra canada
Cheap Sildenafil 100mg Med Men News Buy generic 100mg Viagra online
Viagra generic over the counter: MedMenNews – Viagra generic over the counter
Generic Viagra online: MedMenNews – cheapest viagra
viagra without prescription: sildenafil online – buy Viagra over the counter
Sildenafil 100mg price over the counter sildenafil cheap viagra
Generic Viagra online: buy viagra here – sildenafil online
Sildenafil 100mg price: best price for viagra 100mg – Viagra generic over the counter
order viagra: Med Men News – Generic Viagra for sale
Generic Viagra for sale Med Men News Viagra generic over the counter
sildenafil 50 mg price: MedMenNews – Viagra Tablet price
Viagra without a doctor prescription Canada buy Viagra over the counter Cheap Sildenafil 100mg
buy viagra here: MedMenNews – Viagra generic over the counter
sildenafil online: MedMenNews – Viagra Tablet price
Generic Viagra online cheapest viagra Sildenafil 100mg price
Viagra online price: over the counter sildenafil – Cheap generic Viagra
order viagra: Med Men News – cheapest viagra
Viagra online price: MedMenNews – order viagra
Viagra generic over the counter Med Men News cheap viagra
Viagra Tablet price: Med Men News – viagra without prescription
cheapest viagra: best price for viagra 100mg – Cheapest Sildenafil online
cheapest viagra Med Men News cheap viagra
Cheap Viagra 100mg: Med Men News – cheap viagra
online casino 50 euro eps
Feel free to surf to my web-site … automatenspiele Mit Echtgeld
(Agencialiderdigital.Dev.br)
Viagra online price: Med Men News – sildenafil 50 mg price
Cheap generic Viagra MedMenNews buy viagra here
Generic Viagra for sale: cheap viagra – Viagra Tablet price
Buy Viagra online cheap: order viagra – Cheap generic Viagra
buy Viagra over the counter: Med Men News – Viagra without a doctor prescription Canada
order viagra Cheap generic Viagra online generic sildenafil
Cheapest Sildenafil online: buy Viagra online – Viagra tablet online
sildenafil over the counter buy Viagra online Order Viagra 50 mg online
cheapest viagra: Med Men News – viagra canada
cheapest viagra: MedMenNews – cheap viagra